Men with asymptomatic inflammatory prostatitis do not have symptoms. A health care provider may diagnose asymptomatic inflammatory prostatitis when testing for other urinary tract or reproductive tract disorders. This type of prostatitis does not cause complications and does not need treatment.
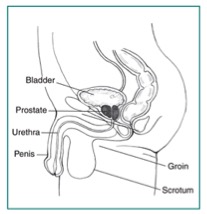
The prostate is a walnut-shaped gland that is part of the male reproductive system. The main function of the prostate is to make a fluid that goes into semen. Prostate fluid is essential for a man’s fertility. The gland surrounds the urethra at the neck of the bladder. The bladder neck is the area where the urethra joins the bladder. The bladder and urethra are parts of the lower urinary tract. The prostate has two or more lobes, or sections, enclosed by an outer layer of tissue, and it is in front of the rectum, just below the bladder. The urethra is the tube that carries urine from the bladder to the outside of the body. In men, the urethra also carries semen out through the penis.
The prostate is a walnut-shaped gland that is part of the male reproductive system.
The causes of prostatitis differ depending on the type.
Chronic prostatitis/chronic pelvic pain syndrome. The exact cause of chronic prostatitis/chronic pelvic pain syndrome is unknown. Researchers believe a microorganism, though not a bacterial infection, may cause the condition. This type of prostatitis may relate to chemicals in the urine, the immune system’s response to a previous urinary tract infection (UTI), or nerve damage in the pelvic area.
Acute and chronic bacterial prostatitis. A bacterial infection of the prostate causes bacterial prostatitis. The acute type happens suddenly and lasts a short time, while the chronic type develops slowly and lasts a long time, often years. The infection may occur when bacteria travel from the urethra into the prostate.
Prostatitis is the most common urinary tract problem for men younger than age 50 and the third most common urinary tract problem for men older than age 50.1 Prostatitis accounts for about two million visits to health care providers in the United States each year.2
Chronic prostatitis/chronic pelvic pain syndrome is the most common and least understood form of prostatitis. Chronic prostatitis/chronic pelvic pain syndrome can occur in men of any age group and affects 10 to 15 percent of the U.S. male population.3
The factors that affect a man’s chances of developing prostatitis differ depending on the type.
Chronic prostatitis/chronic pelvic pain syndrome. Men with nerve damage in the lower urinary tract due to surgery or trauma may be more likely to develop chronic prostatitis/chronic pelvic pain syndrome. Psychological stress may also increase a man’s chances of developing the condition.
Acute and chronic bacterial prostatitis. Men with lower UTIs may be more likely to develop bacterial prostatitis. UTIs that recur or are difficult to treat may lead to chronic bacterial prostatitis.
Each type of prostatitis has a range of symptoms that vary depending on the cause and may not be the same for every man. Many symptoms are similar to those of other conditions.
Chronic prostatitis/chronic pelvic pain syndrome. The main symptoms of chronic prostatitis/chronic pelvic pain syndrome can include pain or discomfort lasting 3 or more months in one or more of the following areas:
· between the scrotum and anus
· the central lower abdomen
· the penis
· the scrotum
· the lower back
Pain during or after ejaculation is another common symptom. A man with chronic prostatitis/chronic pelvic pain syndrome may have pain spread out around the pelvic area or may have pain in one or more areas at the same time. The pain may come and go and appear suddenly or gradually. Other symptoms may include
· pain in the urethra during or after urination.
· pain in the penis during or after urination.
· urinary frequency—urination eight or more times a day. The bladder begins to contract even when it contains small amounts of urine, causing more frequent urination.
· urinary urgency—the inability to delay urination.
· a weak or an interrupted urine stream.
Acute bacterial prostatitis. The symptoms of acute bacterial prostatitis come on suddenly and are severe. Men should seek immediate medical care. Symptoms of acute bacterial prostatitis may include
· urinary frequency
· urinary urgency
· fever
· chills
· a burning feeling or pain during urination
· pain in the genital area, groin, lower abdomen, or lower back
· noctur
· ia—frequent urination during periods of sleep
· nausea and vomiting
· body aches
· urinary retention—the inability to empty the bladder completely
· trouble starting a urine stream
· a weak or an interrupted urine stream
· urinary blockage—the complete inability to urinate
· a UTI—as shown by bacteria and infection-fighting cells in the urine
Chronic bacterial prostatitis. The symptoms of chronic bacterial prostatitis are similar to those of acute bacterial prostatitis, though not as severe. This type of prostatitis often develops slowly and can last 3 or more months. The symptoms may come and go, or they may be mild all the time. Chronic bacterial prostatitis may occur after previous treatment of acute bacterial prostatitis or a UTI. The symptoms of chronic bacterial prostatitis may include
· urinary frequency
· urinary urgency
· a burning feeling or pain during urination
· pain in the genital area, groin, lower abdomen, or lower back
A person may have urinary symptoms unrelated to prostatitis that are caused by bladder problems, UTIs, or benign prostatic hyperplasia. Symptoms of prostatitis also can signal more serious conditions, including prostate cancer.
Men with symptoms of prostatitis should see a health care provider.
Men with the following symptoms should seek immediate medical care:
· complete inability to urinate
· painful, frequent, and urgent need to urinate, with fever and chills
· blood in the urine
· great discomfort or pain in the lower abdomen and urinary tract
A physical exam may help diagnose prostatitis. During a physical exam, a health care provider usually
· examines a patient’s body, which can include checking for
o discharge from the urethra
o enlarged or tender lymph nodes in the groin
o a swollen or tender scrotum
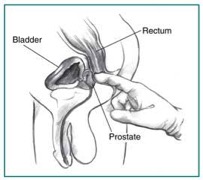
· performs a digital rectal exam
A digital rectal exam, or rectal exam, is a physical exam of the prostate. To perform the exam, the health care provider asks the man to bend over a table or lie on his side while holding his knees close to his chest. The health care provider slides a gloved, lubricated finger into the rectum and feels the part of the prostate that lies next to the rectum. The man may feel slight, brief discomfort during the rectal exam. A health care provider usually performs a rectal exam during an office visit, and the man does not need anesthesia. The exam helps the health care provider see if the prostate is enlarged or tender or has any abnormalities that require more testing.
Many health care providers perform a rectal exam as part of a routine physical exam for men age 40 or older, whether or not they have urinary problems.
A health care provider may refer men to a urologist—a doctor who specializes in the urinary tract and male reproductive system. A urologist uses medical tests to help diagnose lower urinary tract problems related to prostatitis and recommend treatment. Medical tests may include
· urinalysis
· blood tests
· urodynamic tests
· cystoscopy
· transre
· ctal ultrasound
· biopsy
· semen analysis
Urinalysis. Urinalysis involves testing a urine sample. The patient collects a urine sample in a special container in a health care provider’s office or a commercial facility. A health care provider tests the sample during an office visit or sends it to a lab for analysis. For the test, a nurse or technician places a strip of chemically treated paper, called a dipstick, into the urine. Patches on the dipstick change color to indicate signs of infection in urine.
The health care provider can diagnose the bacterial forms of prostatitis by examining the urine sample with a microscope. The health care provider may also send the sample to a lab to perform a culture. In a urine culture, a lab technician places some of the urine sample in a tube or dish with a substance that encourages any bacteria present to grow; once the bacteria have multiplied, a technician can identify them.
Blood tests. Blood tests involve a health care provider drawing blood during an office visit or in a commercial facility and sending the sample to a lab for analysis. Blood tests can show signs of infection and other prostate problems, such as prostate cancer.
Urodynamic tests. Urodynamic tests include a variety of procedures that look at how well the bladder and urethra store and release urine. A health care provider performs urodynamic tests during an office visit or in an outpatient center or a hospital. Some urodynamic tests do not require anesthesia; others may require local anesthesia. Most urodynamic tests focus on the bladder’s ability to hold urine and empty steadily and completely and may include the following:
· uroflowmetry, which measures how rapidly the bladder releases urine
· postvoid residual measurement, which evaluates how much urine remains in the bladder after urination
More information is provided in the NIDDK health topic, Urodynamic Testing.
Cystoscopy. Cystoscopy is a procedure that uses a tubelike instrument, called a cystoscope, to look inside the urethra and bladder. A urologist inserts the cystoscope through the opening at the tip of the penis and into the lower urinary tract. He or she performs cystoscopy during an office visit or in an outpatient center or a hospital. He or she will give the patient local anesthesia. In some cases, the patient may require sedation and regional or general anesthesia. A urologist may use cystoscopy to look for narrowing, blockage, or stones in the urinary tract.
Transrectal ultrasound. Transrectal ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. The health care provider can move the transducer to different angles to make it possible to examine different organs. A specially trained technician performs the procedure in a health care provider’s office, an outpatient center, or a hospital, and a radiologist—a doctor who specializes in medical imaging—interprets the images; the patient does not require anesthesia. Urologists most often use transrectal ultrasound to examine the prostate. In a transrectal ultrasound, the technician inserts a transducer slightly larger than a pen into the man’s rectum next to the prostate. The ultrasound image shows the size of the prostate and any abnormalities, such as tumors. Transrectal ultrasound cannot reliably diagnose prostate cancer.
Biopsy. Biopsy is a procedure that involves taking a small piece of prostate tissue for examination with a microscope. A urologist performs the biopsy in an outpatient center or a hospital. He or she will give the patient light sedation and local anesthetic; however, in some cases, the patient will require general anesthesia. The urologist uses imaging techniques such as ultrasound, a computerized tomography scan, or magnetic resonance imaging to guide the biopsy needle into the prostate. A pathologist—a doctor who specializes in examining tissues to diagnose diseases—examines the prostate tissue in a lab. The test can show whether prostate cancer is present.
Semen analysis. Semen analysis is a test to measure the amount and quality of a man’s semen and sperm. The man collects a semen sample in a special container at home, a health care provider’s office, or a commercial facility. A health care provider analyzes the sample during an office visit or sends it to a lab for analysis. A semen sample can show blood and signs of infection.
Chronic prostatitis/chronic pelvic pain syndrome. Treatment for chronic prostatitis/chronic pelvic pain syndrome aims to decrease pain, discomfort, and inflammation. A wide range of symptoms exists and no single treatment works for every man. Although antibiotics will not help treat nonbacterial prostatitis, a urologist may prescribe them, at least initially, until the urologist can rule out a bacterial infection. A urologist may prescribe other medications:
· silodo
· sin (Rapaflo)
· 5-alpha reductase inhibitors such as finasteride (Proscar) and dutasteride (Avodart)
· nonsteroidal anti-inflammatory drugs—also called NSAIDs—such as aspirin, ibuprofen, and naproxen sodium
· glycosaminogly
· cans such as chondroitin sulfate
· muscle relaxants such as cyclobenzaprine (Amrix, Flexeril) and clonazepam (Klonopin)
· neuromodulators such as amitriptyline, nortriptyline (Aventyl, Pamelor), and pregabalin (Lyrica)
Alternative treatments may include
· warm baths, called sitz baths
· local heat therapy with hot water bottles or heating pads
· physical therapy, such as
o Kegel exercises—tightening and relaxing the muscles that hold urine in the bladder and hold the bladder in its proper position. Also called pelvic muscle exercises.
o myofascial release—pressing and stretching, sometimes with cooling and warming, of the muscles and soft tissues in the lower back, pelvic region, and upper legs. Also known as myofascial trigger point release.
· relaxation exercises
· biofeedback
· phytotherapy with plant extracts such as quercetin, bee pollen, and saw palmetto
· acupuncture
To help ensure coordinated and safe care, people should discuss their use of complementary and alternative medical practices, including their use of dietary supplements, with their health care provider. Read more at www.nccam.nih.gov .
For men whose chronic prostatitis/chronic pelvic pain syndrome symptoms are affected by psychological stress, appropriate psychiatric treatment and stress reduction may reduce the recurrence of symptoms.
To help measure the effectiveness of treatment, a urologist may ask a series of questions from a standard questionnaire called the National Institutes of Health (NIH) Chronic Prostatitis Symptom Index. The questionnaire helps a urologist assess the severity of symptoms and how they affect the man’s quality of life. A urologist may ask questions several times, such as before, during, and after treatment.
Acute bacterial prostatitis. A urologist treats acute bacterial prostatitis with antibiotics. The antibiotic prescribed may depend on the type of bacteria causing the infection. Urologists usually prescribe oral antibiotics for at least 2 weeks. The infection may come back; therefore, some urologists recommend taking oral antibiotics for 6 to 8 weeks. Severe cases of acute prostatitis may require a short hospital stay so men can receive fluids and antibiotics through an intravenous (IV) tube. After the IV treatment, the man will need to take oral antibiotics for 2 to 4 weeks. Most cases of acute bacterial prostatitis clear up completely with medication and slight changes to diet. The urologist may recommend
· avoiding or reducing intake of substances that irritate the bladder, such as alcohol, caffeinated beverages, and acidic and spicy foods
· increasing intake of liquids—64 to 128 ounces per day—to urinate often and help flush bacteria from the bladder
Chronic bacterial prostatitis. A urologist treats chronic bacterial prostatitis with antibiotics; however, treatment requires a longer course of therapy. The urologist may prescribe a low dose of antibiotics for up to 6 months to prevent recurrent infection. The urologist may also prescribe a different antibiotic or use a combination of antibiotics if the infection keeps coming back. The urologist may recommend increasing intake of liquids and avoiding or reducing intake of substances that irritate the bladder.
A urologist may use alpha blockers that treat chronic prostatitis/chronic pelvic pain syndrome to treat urinary retention caused by chronic bacterial prostatitis. These medications help relax the bladder muscles near the prostate and lessen symptoms such as painful urination. Men may require surgery to treat urinary retention caused by chronic bacterial prostatitis. Surgically removing scar tissue in the urethra often improves urine flow and reduces urinary retention.
Researchers have not found that eating, diet, and nutrition play a role in causing or preventing prostatitis. During treatment of bacterial prostatitis, urologists may recommend increasing intake of liquids and avoiding or reducing intake of substances that irritate the bladder. Men should talk with a health care provider or dietitian about what diet is right for them.
· Prostatitis is a frequently painful condition that involves inflammation of the prostate and sometimes the areas around the prostate.
· Scientists have identified four types of prostatitis:
o chronic prostatitis/chronic pelvic pain syndrome
o acute bacterial prostatitis
o chronic bacterial prostatitis
o asymptomatic inflammatory prostatitis
· The prostate is a walnut-shaped gland that is part of the male reproductive system.
· The causes of prostatitis differ depending on the type.
· Prostatitis is the most common urinary tract problem for men younger than age 50 and the third most common urinary tract problem for men older than age 50.
· Each type of prostatitis has a range of symptoms that vary depending on the cause and may not be the same for every man. Many symptoms are similar to those of other conditions.
· The complications of prostatitis may include
o bacterial infection in the bloodstream
o prostatic abscess—a pus-filled cavity in the prostate
o sexual dysfunction
o inflammation of reproductive organs near the prostate
· A health care provider diagnoses prostatitis based on
o a personal and family history
o a physical exam
o medical tests
· A health care provider may have to rule out other conditions that cause similar signs and symptoms before diagnosing prostatitis.
· Treatment depends on the type of prostatitis.
· Treatment for chronic prostatitis/chronic pelvic pain syndrome aims to decrease pain, discomfort, and inflammation.
· A urologist treats acute bacterial prostatitis with antibiotics.
· A urologist treats chronic bacterial prostatitis with antibiotics; however, treatment requires a longer course of therapy.
Pleurisy (PLUR-ih-se) is a condition in which the pleura is inflamed. The pleura is a membrane that consists of two large, thin layers of tissue. One layer wraps around the outside of your lungs. The other layer lines the inside of your chest cavity.
Between the layers of tissue is a very thin space called the pleural space. Normally this space is filled with a small amount of fluid—about 4 teaspoons full. The fluid helps the two layers of the pleura glide smoothly past each other as you breathe in and out.
Pleurisy occurs if the two layers of the pleura become irritated and inflamed. Instead of gliding smoothly past each other, they rub together every time you breathe in. The rubbing can cause sharp pain.
Many conditions can cause pleurisy, including viral infections.
Other Pleural Disorders
Pneumothorax
Air or gas can build up in the pleural space. When this happens, it's called a pneumothorax (noo-mo-THOR-aks). A lung disease or acute lung injury can cause a pneumothorax.
Some lung procedures also can cause a pneumothorax. Examples include lung surgery, drainage of fluid with a needle, bronchoscopy (bron-KOS-ko-pee), and mechanical ventilation.
Sometimes the cause of a pneumothorax isn't known.
The most common symptoms of a pneumothorax are sudden pain in one side of the lung and shortness of breath. The air or gas in the pleural space also can put pressure on the lung and cause it to collapse.
Pleurisy and Pneumothorax
A small pneumothorax may go away without treatment. A large pneumothorax may require a procedure to remove air or gas from the pleural space.
A very large pneumothorax can interfere with blood flow through your chest and cause your blood pressure to drop. This is called a tension pneumothorax.
Pleural Effusion
In some cases of pleurisy, excess fluid builds up in the pleural space. This is called a pleural effusion. A lot of extra fluid can push the pleura against your lung until the lung, or part of it, collapses. This can make it hard for you to breathe.
Sometimes the extra fluid gets infected and turns into an abscess. When this happens, it's called an empyema (em-pi-E-ma).
You can develop a pleural effusion even if you don't have pleurisy. For example, pneumonia, (nu-MO-ne-ah), heart failure, cancer, or pulmonary embolism (PULL-mun-ary EM-bo-lizm) can lead to a pleural effusion.
Hemothorax
Blood also can build up in the pleural space. This condition is called a hemothorax (he-mo-THOR-aks). An injury to your chest, chest or heart surgery, or lung or pleural cancer can cause a hemothorax.
A hemothorax can put pressure on the lung and cause it to collapse. A hemothorax also can cause shock. In shock, not enough blood and oxygen reach your body's vital organs.
Outlook
Pleurisy and other pleural disorders can be serious, depending on their causes. If the condition that caused the pleurisy or other pleural disorder isn't too serious and is diagnosed and treated early, you usually can expect a full recovery.
Other Names for Pleurisy and Other Pleural Disorders
Pleurisy also is called pleuritis and pleuritic chest pain.
Pleural effusion also is called fluid in the chest and pleural fluid.
Pneumothorax also is called air around the lung and air outside the lung
What Causes Pleurisy and Other Pleural Disorders?
Pleurisy
Many conditions can cause pleurisy. Viral infections are likely the most common cause. Other causes of pleurisy include:
Bacterial infections, such as pneumonia (nu-MO-ne-ah) and tuberculosis, and infections from fungi or parasites
Pulmonary embolism, a blood clot that travels through the blood vessels to the lungs
Autoimmune disorders, such as lupus and rheumatoid arthritis
Cancer, such as lung cancer, lymphoma, and mesothelioma (MEZ-o-thee-lee-O-ma)
Lung diseases, such as LAM (lymphangioleiomyomatosis) or asbestosis (as-bes-TO-sis)
Inflammatory bowel disease
Familial Mediterranean fever, an inherited condition that often causes fever and swelling in the abdomen or lungs
Other causes of pleurisy include chest injuries, pancreatitis (an inflamed pancreas), and reactions to certain medicines. Reactions to certain medicines can cause a condition similar to lupus. These medicines include procainamide, hydralazine, and isoniazid.
Sometimes doctors can't find the cause of pleurisy.
Pneumothorax
Lung diseases or acute lung injury can make it more likely that you will develop a pneumothorax (a buildup of air or gas in the pleural space). Such lung diseases may includeCOPD (chronic obstructive pulmonary disease), tuberculosis, and LAM.
Surgery or a chest injury also may cause a pneumothorax.
You can develop a pneumothorax without having a recognized lung disease or chest injury. This is called a spontaneous pneumothorax. Smoking increases your risk of spontaneous pneumothorax. Having a family history of the condition also increases your risk.
Pleural Effusion
The most common cause of a pleural effusion (a buildup of fluid in the pleural space) is heart failure. Lung cancer, LAM, pneumonia, tuberculosis, and other lung infections also can lead to a pleural effusion.
Sometimes kidney or liver disease can cause fluid to build up in the pleural space. Asbestosis, sarcoidosis (sar-koy-DO-sis), and reactions to some medicines also can lead to a pleural effusion.
Hemothorax
An injury to the chest, chest or heart surgery, or lung or pleural cancer can cause a hemothorax (buildup of blood in the pleural space).
A hemothorax also can be a complication of an infection (for example, pneumonia), tuberculosis, or a spontaneous pneumothorax.
What Are the Signs and Symptoms of Pleurisy and Other Pleural Disorders
Pleurisy
The main symptom of pleurisy is a sharp or stabbing pain in your chest that gets worse when you breathe in deeply or cough or sneeze.
The pain may stay in one place or it may spread to your shoulders or back. Sometimes the pain becomes a fairly constant dull ache.
Depending on what's causing the pleurisy, you may have other symptoms, such as:
Shortness of breath or rapid, shallow breathing
Coughing
Fever and chills
Unexplained weight loss
Pneumothorax
The symptoms of pneumothorax include:
Sudden, sharp chest pain that gets worse when you breathe in deeply or cough
Shortness of breath
Chest tightness
Easy fatigue (tiredness)
A rapid heart rate
A bluish tint to the skin caused by lack of oxygen
Other symptoms of pneumothorax include flaring of the nostrils; anxiety, stress, and tension; and hypotension (low blood pressure).
Pleural Effusion
Pleural effusion often has no symptoms.
Hemothorax
The symptoms of hemothorax often are similar to those of pneumothorax. They include:
How Are Pleurisy and Other Pleural Disorders Diagnosed?
Your doctor will diagnose pleurisy or another pleural disorder based on your medical history, a physical exam, and test results.
Your doctor will want to rule out other causes of your symptoms. He or she also will want to find the underlying cause of the pleurisy or other pleural disorder so it can be treated.
Medical History
Your doctor may ask detailed questions about your medical history. He or she likely will ask you to describe any pain, especially:
What it feels like
Where it's located and whether you can feel it in your arms, jaw, or shoulders
When it started and whether it goes away and then comes back
What makes it better or worse
Your doctor also may ask whether you have other symptoms, such as shortness of breath,coughing, or palpitations. Palpitations are feelings that your heart is skipping a beat, fluttering, or beating too hard or fast.
Your doctor also may ask whether you've ever:
Had heart disease.
Smoked.
Traveled to places where you may have been exposed to tuberculosis.
Had a job that exposed you to asbestos. Asbestos is a mineral that, at one time, was widely used in many industries.
Your doctor also may ask about medicines you take or have taken. Reactions to some medicines can cause pleurisy or other pleural disorders.
Physical Exam
Your doctor will listen to your breathing with a stethoscope to find out whether your lungs are making any abnormal sounds.
If you have pleurisy, the inflamed layers of the pleura make a rough, scratchy sound as they rub against each other when you breathe. Doctors call this a pleural friction rub. If your doctor hears the friction rub, he or she will know that you have pleurisy.
If you have a pleural effusion, fluid buildup in the pleural space will prevent a friction rub. But if you have a lot of fluid, your doctor may hear a dull sound when he or she taps on your chest. Or, he or she may have trouble hearing any breathing sounds.
Muffled or dull breathing sounds also can be a sign of a pneumothorax (a buildup of air or gas in the pleural space).
Diagnostic Tests
Depending on the results of your physical exam, your doctor may recommend tests.
Chest X Ray
A chest x ray is a painless test that creates a picture of the structures in your chest, such as your heart, lungs, and blood vessels. This test may show air or fluid in the pleural space.
A chest x ray also may show what's causing a pleural disorder—for example, pneumonia, a fractured rib, or a lung tumor.
Sometimes a chest x ray is taken while you lie on your side. This position can show fluid that didn't appear on an x ray taken while you were standing.
Chest CT Scan
A chest computed tomography (to-MOG-rah-fee) scan, or chest CT scan, is a painless test that creates precise pictures of the structures in your chest.
This test provides a computer-generated picture of your lungs that can show pockets of fluid. A chest CT scan also may show signs of pneumonia, a lung abscess, a tumor, or other possible causes of pleural disorders.
Ultrasound
This test uses sound waves to create pictures of your lungs. An ultrasound may show where fluid is located in your chest. The test also can show some tumors.
Chest MRI
A chest magnetic resonance imaging scan, or chest MRI, uses radio waves, magnets, and a computer to created detailed pictures of the structures in your chest. This test can show pleural effusions and tumors.
This test also is called a magnetic resonance (MR) scan or a nuclear magnetic resonance (NMR) scan.
Blood Tests
Blood tests can show whether you have an illness that increases your risk of pleurisy or another pleural disorder. Such illnesses include bacterial or viral infections, pneumonia, pancreatitis (an inflamed pancreas), kidney disease, or lupus.
Arterial Blood Gas Test
For this test, a blood sample is taken from an artery, usually in your wrist. The blood's oxygen and carbon dioxide levels are checked. This test shows how well your lungs are taking in oxygen.
Thoracentesis
Once your doctor knows whether fluid has built up in the pleural space and where it is, he or she can remove a sample for testing. This is done using a procedure called thoracentesis (THOR-ah-sen-TE-sis).
During the procedure, your doctor inserts a thin needle or plastic tube into the pleural space and draws out the excess fluid. After the fluid is removed from your chest, it's sent for testing.
The risks of thoracentesis—such as pain, bleeding, and infection—usually are minor. They get better on their own, or they're easily treated. Your doctor may do a chest x ray after the procedure to check for complications.
Fluid Analysis
The fluid removed during thoracentesis is examined under a microscope. It's checked for signs of infection, cancer, or other conditions that can cause fluid or blood to build up in the pleural space.
Biopsy
Your doctor may suspect that tuberculosis or cancer has caused fluid to build up in your pleural space. If so, he or she may want to look at a small piece of the pleura under a microscope.
To take a tissue sample, your doctor may do one of the following procedures:
Insert a needle into your chest to remove a small sample of the pleura's outer layer.
Insert a tube with a light on the end (endoscope) into tiny cuts in your chest wall so that he or she can see the pleura. Your doctor can then snip out small pieces of tissue. This procedure must be done in a hospital. You'll be given medicine to make you sleep during the procedure.
Snip out a sample of the pleura through a small cut in your chest wall. This is called an open pleural biopsy. It's usually done if the sample from the needle biopsy is too small for an accurate diagnosis. This procedure must be done in a hospital. You'll be given medicine to make you sleep during the procedure.
How Are Pleurisy and Other Pleural Disorders Treated?
Pleurisy and other pleural disorders are treated with procedures, medicines, and other methods. The goals of treatment include:
Relieving symptoms
Removing the fluid, air, or blood from the pleural space (if a large amount is present)
Treating the underlying condition
Relieving Symptoms
To relieve pleurisy symptoms, your doctor may recommend:
Acetaminophen or anti-inflammatory medicines (such as ibuprofen) to control pain.
Lying on your painful side. This might make you more comfortable.
Breathing deeply and coughing to clear mucus as the pain eases. Otherwise, you may develop pneumonia.
Getting plenty of rest.
Removing Fluid, Air, or Blood From the Pleural Space
Your doctor may recommend removing fluid, air, or blood from your pleural space to prevent a lung collapse.
The procedures used to drain fluid, air, or blood from the pleural space are similar.
During thoracentesis, your doctor will insert a thin needle or plastic tube into the pleural space. An attached syringe will draw fluid out of your chest. This procedure can remove more than 6 cups of fluid at a time.
If your doctor needs to remove a lot of fluid, he or she may use a chest tube. Your doctor will inject a painkiller into the area of your chest wall where the fluid is. He or she will then insert a plastic tube into your chest between two ribs. The tube will be connected to a box that suctions out the fluid. Your doctor will use a chest x ray to check the tube's position.
Your doctor also can use a chest tube to drain blood and air from the pleural space. This process can take several days. The tube will be left in place, and you'll likely stay in the hospital during this time.
Sometimes the fluid in the pleural space contains thick pus or blood clots. It may form a hard skin or peel, which makes the fluid harder to drain. To help break up the pus or blood clots, your doctor may use a chest tube to deliver medicines called fibrinolytics to the pleural space. If the fluid still won't drain, you may need surgery.
If you have a small, persistent air leak into the pleural space, your doctor may attach a one-way valve to the chest tube. The valve allows air to exit the pleural space, but not reenter. Using this type of valve may allow you to continue your treatment from home.
Treat the Underlying Condition
The fluid sample that was removed during thoracentesis will be checked under a microscope. This can tell your doctor what's causing the fluid buildup, and he or she can decide the best way to treat it.
If the fluid is infected, treatment will involve antibiotics and drainage. If you have tuberculosis or a fungal infection, treatment will involve long-term use of antibiotics or antifungal medicines.
If tumors in the pleura are causing fluid buildup, the fluid may quickly build up again after it's drained. Sometimes antitumor medicines will prevent further fluid buildup. If they don't, your doctor may seal the pleural space. Sealing the pleural space is called pleurodesis (plur-OD-eh-sis).
For this procedure, your doctor will drain all of the fluid out of your chest through a chest tube. Then he or she will push a substance through the chest tube into the pleural space. The substance will irritate the surface of the pleura. This will cause the two layers of the pleura to stick together, preventing more fluid from building up.
Chemotherapy or radiation treatment also may be used to reduce the size of the tumors.
If heart failure is causing fluid buildup, treatment usually includes diuretics (medicines that help reduce fluid buildup) and other medicines.
Dehydration means your body does not have as much water and fluids as it should.
Dehydration can be mild, moderate, or severe based on how much of the body's fluid is lost or not replenished. When it is severe, dehydration is a life-threatening emergency.
Dehydration in sick children is often a combination of refusing to eat or drink anything and losing fluid from vomiting, diarrhea, or fever.
Infants and children are more likely to become dehydrated than adults because they weigh less and their bodies turn over water and electrolytes more quickly. The elderly and people with illnesses are also at higher risk.
You may also have vomiting, diarrhea, or the feeling that you "can't keep anything down." All of these can be causing the dehydration.
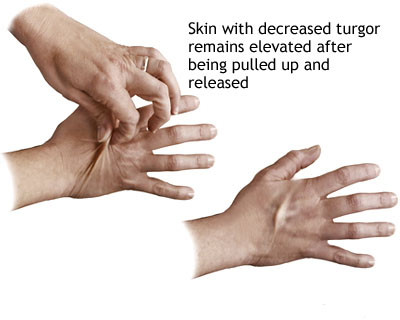
A decrease in skin turgor is indicated when the skin (on the back of the hand for an adult or on the abdomen for a child) is pulled up for a few seconds and does not return to its original state. A decrease in skin turgor is a late sign of dehydration.
Poor skin turgor -- the skin may not be as elastic as normal and sag back into position slowly when the health care provider pinches it up into a fold (normally, skin springs right back into place)
Drinking fluids is usually enough for mild dehydration. It is better to drink small amounts of fluid often (using a teaspoon or syringe for an infant or child), instead of trying to force large amounts of fluid at one time. Drinking too much fluid at once can bring on more vomiting.
Electrolyte solutions or freezer pops are very effective. These are available at pharmacies. Sports drinks contain a lot of sugar and can cause or worsen diarrhea. In infants and children, avoid using water as the primary replacement fluid.
Intravenous fluids and a hospital stay may be needed for moderate to severe dehydration. The health care provider will try to identify and then treat the cause of the dehydration.
Most cases of stomach viruses (also called viral gastroenteritis) tend to get better on their own after a few days. See also: Diarrhea
Even when you are healthy, drink plenty of fluids every day. Drink more when the weather is hot or you are exercising.
Carefully monitor someone who is ill, especially an infant, child, or older adult. If you believe that the person is getting dehydrated, call your health care provider before the person becomes dehydrated. Begin fluid replacement as soon as vomiting and diarrhea start -- DO NOT wait for signs of dehydration.
Always encourage a person who is sick to drink fluids. Remember that fluid needs are greater with a fever, vomiting, or diarrhea. The easiest signs to monitor are urine output (there should be frequent wet diapers or trips to the bathroom), saliva in the mouth, and tears when crying.
What is traveler's diarrhea?
People get traveler's diarrhea by eating food and drinking water that contain germs. People can get this illness in areas of the world where the drinking water is not clean.
People who live these areas often drink tap water that contains these germs, but they do not get diarrhea. This is because their bodies are used to the germs. In the same way, cooks and food handlers may have the germs that cause traveler's diarrhea on their hands, but they may not get sick themselves. When people travel to a new place, they are more likely to become sick, because they lack protective antibodies (infection-fighting agents in the blood) that attack these germs.
How can I tell if I have traveler's diarrhea?
You may have traveler's diarrhea if you have at least 3 loose stools in 24 hours. You may also have one or more of the following symptoms:
Even if you don't treat traveler's diarrhea, it will usually go away in 4 to 5 days. You should drink plenty of clear liquids to replace lost fluids due to the diarrhea. Taking medicine to treat traveler's diarrhea may make you feel better more quickly. It often is treated with antibiotics (medicines that kill bacteria). To get antibiotics, you need a prescription from your doctor.
You also can take a medicine called loperamide (brand name: Imodium). However, if you have bloody diarrhea, you should not take this medicine without also taking an antibiotic.
Children, pregnant women, older adults and other people who get dehydrated easily should drink rehydration solutions. Rehydration solutions help replace the fluid you lose while you are sick. You can buy packets of rehydration salts (to be mixed with safe water) at camping/outdoor stores or drug stores.
When should I contact my doctor?
If your child has a fever higher than 102°F, is dehydrated, has blood in the stool or vomits several times, he or she should see a doctor right away.
If treating your traveler's diarrhea isn't helping you to feel better, talk to your doctor.
How can I avoid traveler's diarrhea?
When you will be traveling to an area where the water may not be clean, see your doctor 4 to 6 weeks before your trip. Your doctor may want to give you some medicines, such as antibiotics or shots, to protect you from illness while you are away. During your trip, be careful about the following things:
Do not drink tap water and do not use it to brush your teeth.
Do not drink bottled water if the seal on the bottle has been broken.
Do not use ice unless you're sure it's made from purified water.
Do not drink milk or eat dairy products that have not been pasteurized (heated to a temperature that kills all germs).
Do not eat raw fruits or vegetables unless they can be peeled and you are the one who peels them.
Do not eat cut-up fruit salad.
Do not eat lettuce or other leafy raw vegetables (such as spinach).
Do not eat raw or rare (slightly cooked) meat or fish.
Do not eat food from people who sell it on the street.
Boiling water will kill the germs that cause diarrhea, making the water safe to drink. Boil water vigorously for 1 minute and allow it to cool to room temperature (do not add ice). When traveling in high altitudes (6,562 feet or higher), boil water for 3 minutes.
What is safe to eat or drink?
When you are in a place where you could get traveler's diarrhea, it is probably safe to eat or drink the following:
Soft drinks that are carbonated (such as cola).
Hot drinks, such as tea or coffee.
Carbonated or noncarbonated bottled water, as long as you are the one who breaks the seal on the bottle.
Raw fruits or vegetables that can be peeled, as long as you are the one who peels them.
Food that is served hot.
Meat that is well cooked.
Questions to Ask Your Doctor
Is there medicine I can take to prevent traveler’s diarrhea?
Is traveler’s diarrhea common in the country I’m traveling to?
If I get traveler’s diarrhea, who should I contact and when?
Aspergillosis is caused by a fungus called Aspergillus. The fungus is often found growing on dead leaves, stored grain, compost piles, or in other decaying vegetation. It can also be found on marijuana leaves.
Although most people are often exposed to Aspergillus, infections caused by the fungus rarely occur in people who have a healthy immune system.
There are several forms of aspergillosis:
Allergic pulmonary aspergillosis is an allergic reaction to the fungus. This infection usually develops in people who already have lung problems such as asthma or cystic fibrosis.
Invasive pulmonary aspergillosis is a serious infection with pneumonia. It can spread to other parts of the body. This infection occurs most often in people with a weakened immune system. This can be from cancer, AIDS, leukemia, an organ transplant, chemotherapy, or other conditions or drugs that lower the number or function of white blood cells or weaken the immune system.
A fungus ball is usually not treated with antifungal medicines unless there is bleeding into the lung tissue. In such a case, surgery and medicines are needed.
Invasive aspergillosis is treated with several weeks of an antifungal medicine. It can be given by mouth or IV (into a vein). Endocarditis caused by Aspergillus is treated by surgically removing the infected heart valves. Long-term antifungal drugs are also needed.
Allergic aspergillosis is treated with drugs that suppress the immune system (immunosuppressive drugs), such as prednisone.
With treatment, people with allergic aspergillosis usually get better over time. It is common for the disease to come back (relapse) and need repeat treatment.
If invasive aspergillosis does not get better with drug treatment, it eventually leads to death. The outlook for invasive aspergillosis also depends on the person's underlying disease and immune system health.
Precautions should be taken when using medicines that suppress the immune system. Preventing HIV/AIDS also prevents certain diseases, including aspergillosis, that are associated with a damaged or weakened immune system.
Toxic shock syndrome is caused by a toxin produced by certain types of Staphylococcus bacteria. A similar syndrome, called toxic shock-like syndrome (TSLS), can be caused by Streptococcal bacteria. Not all staph or strep infections cause toxic shock syndrome.
Although the earliest cases of toxic shock syndrome involved women who were using tampons during their periods (menstruation), today less than half of current cases are associated with such events. Toxic shock syndrome can also occur with skin infections, burns, and after surgery. The condition can also affect children, postmenopausal women, and men.
Risk factors include:
Recently having a baby
Staphylococcus aureus (S. aureus) infection, commonly called a Staph infection
Foreign bodies or packings (such as those used to stop nosebleeds)
Menstruation
Surgery
Tampon use (particularly if you leave one in for a long time)
Widespread red rash that looks like a sunburn -- skin peeling occurs 1 or 2 weeks after the rash, particularly on the palms of the hand or bottom of the feet
The diagnosis is based on several criteria: fever, low blood pressure, a rash that peels after 1-2 weeks, and problems with the function of at least three organs.
In some cases, blood cultures may be positive for growth of S. aureus.
Any foreign materials, such as tampons, vaginal sponges, or nasal packing, will be removed. Sites of infection (such as a surgical wound) will be drained.
The goal of treatment is to maintain important body functions. This may include:
Antibiotics for any infection (may be given through an IV)
Dialysis (if severe kidney problems are present)
Fluids through a vein (IV)
Medicines to control blood pressure
Intravenous gamma globulin in severe cases
Staying in the hospital intensive care unit (ICU) for monitoring
Toxic shock syndrome is a medical emergency. Seek immediate medical attention if you develop a rash, fever, and feel ill, particularly during menstruation and tampon use or if you have had recent surgery.
Menstrual toxic shock syndrome can be prevented by avoiding the use of highly absorbent tampons. You can reduce your risk by changing tampons more frequently and using tampons only once in a while (not regularly) during menstruation.
Сүндетке отырғызылмаған ерлерде пенистің ұшы «күпек» атауымен белгілі тері қабықшамен жабылған. Фимоз кезінде күпектің тарылуы пайда болады, ол жыныстық мүшенің ұшында тығыз тартылып, қайтадан орнына еркін қайта алмайды. Фимоз табиғи көрініс болуы мүмкін. Мысалы, 4 жасқа дейінгі ұлдарда әдетте, күпекті ысыру қиын. Жас адамдарда, ерлерде фимоз көбінесе күпектің қабынуына (баланит) немесе қант диабеті секілді басқа ауруларға байланысты болады.
Парафимоз күпек жыныстық мүшенің ұшынан тыс ысырылып, оны қысқанда пайда болады. Күпек өзінің бастапқы жағдайына қайтпайды және пенистің ұшын жаппайды. Бұл ісінудің, ауырсынудың, пенистің ұшына қан келуінің шектелуіне апаруы мүмкін. Егер күпек өзінің табиғи орналасу жағдайына қайтпаса, күрделі асқынулар пайда болуы мүмкін.
Фимоз, әдетте, ауырсынусыз өтеді. Дегенмен, күпектің тарылуында несеп шығару немесе жыныстық қызметте қиындықтар пайда болуы мүмкін. Сонымен қатар, фимоз кезінде ерлерге күпектің астындағы теріні тазалау қиынға түседі, бұл инфекциялардың пайда болуына ықпал етеді.
Парафимоз күпектің және жыныстық мүшенің ұшының ауырсынып, ісінуімен сипатталады. Пенистің ұшына қан келуінің ауыр тежелуі туралы күңгірт-күлгін түсіне қарап айтуға болады, бұл әдетте, шұғыл медициналық жәрдемді қажет етеді.
Жеке гигиенаны мұқият қадағалау арқылы фимоздың алдын алуға болады. Ол үшін шомылу кезінде күпекті толығымен ысырып, астындағы теріні мұқият тазарту қажет.
Күпектің жыныстық мүшеден тыс ысырылуында әрдайым мұқият түрде бастапқы орналасу жағдайына қайтарып отырсаңыз, парафимоздың алдын алуға болады. Парафимоз пайда болуында, оның қайталанбауы үшін науқастарға сүндетке отырғызылу ұсынылады.
Фимоздың симптомсыз өтуі емдеуді қажет етпейді. Бұл әсіресе, балалар үшін дұрыс. Егер ұлдарда фимоз өтпейтін болса, немесе несеп шығаруға / гигиенаға қатысты мәселелер пайда болса, гидрокортизон секілді емдейтін жақпа майларды қолдану тиімді болуы мүмкін.
Жасөспірімдер мен ерлерде аурудың алдын алу үшін жеке гигиенаны қадағалау және инфекцияларды уақытылы емдеу жеткілікті болуы мүмкін. Қалған жағдайларда, тұрақты симптомдардың болуында да түзету операциясын (сүндетке отырғызу) жасау қажет.
Егер парафимоз кезінде күпек жыныстық мүшеден тыс ысырылатын болса, оны қысатын болса, төтенше жағдай орын алады, бұл кезде шұғыл медициналық жәрдем қажет. Дәрігер шұғыл түрде күпекті кесуі немесе сүндетке отырғызуды өткізуі мүмкін.
Көптеген ерлерде фимоз күрделі мәселеге айналмайды, емдеуді қажет етпейді. Дегенмен, жағдай өздігінше оңалмайды.
Жоғарыда аталғандай, кейде парафимоз шұғыл медициналық жәрдемді қажет етеді. Егер шұғыл медициналық жәрдемге жүгінбесеңіз, жыныстық мүшенің ұшының қайтымсыз зақымдануы орын алуы мүмкін.
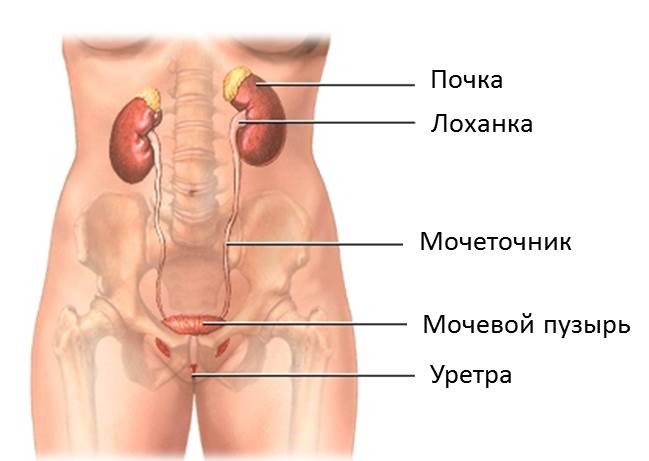
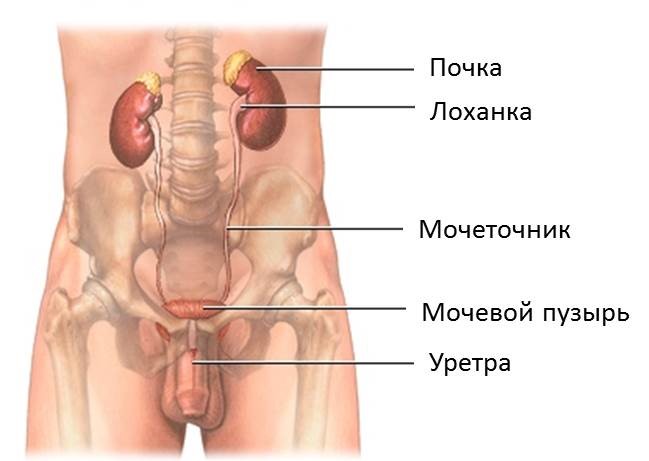
Несеп шығару жолдарының жүйесі – организмнен алмасу заттектері және артық сұйықтық шығарылатын жүйе. Несеп шығару жүйесіне жататындар: бүйректер, несепағарлар, несепқап және үрпі. Несеп шығару жолдарының инфекциясы (НШЖИ), мысалы, цистит және уретрит, организмнің инфекцияларының ішінде кездесу жиілігі бойынша екінші орында.
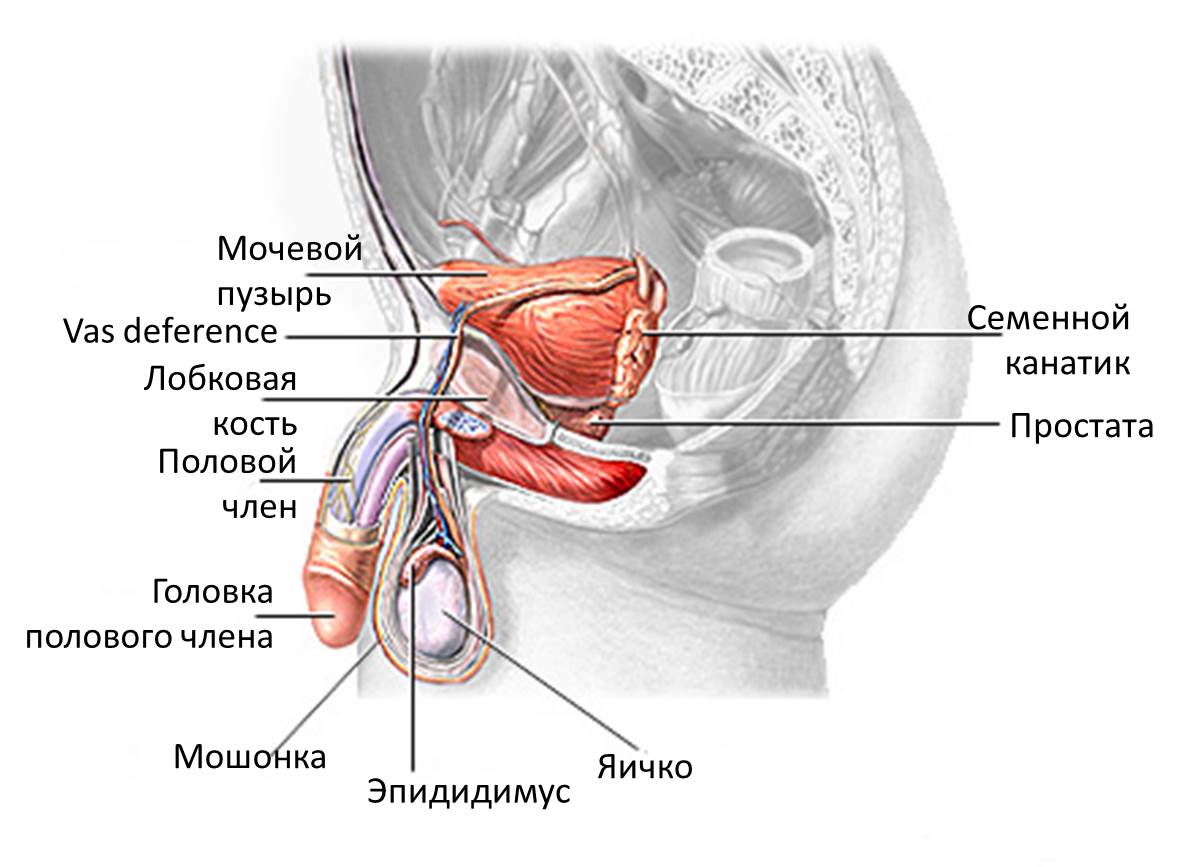
Әйелдердің несеп-жыныс жүйесі Ерлердің несеп-жыныс жүйесі
Несептің сасықтығы, тұнба немесе түсінің қызылдау болуы
Арқадағы немесе қабырға астындағы ауырсыну
Кез келген жастағы адам НШЖИ ауруларына шалдығуы мүмкін. Бірақ, әйелдер ерлерден төрт еседей жиі ауырады. Сондай-ақ, диабет, жұлынның зақымы, немесе несеп катетері болғанда аурудың жоғары қаупі орын алады.
Дисменорея – әйелдердің етеккір алдында немесе басталуында түйілуді немесе ауырсынуды сезінуін сипаттайтын медициналық термин. Бұл күрделі ауырсыну емес.
Етеккірлік түйілу іште, белде, бөкседе немесе бөксенің ішкі жағында батып ауырсыну түрінде сезіледі. Ауырсыну етеккір алдында немесе осы кезеңнің басында басталуы және 1-3 күн созылуы мүмкін. Ауырсыну қарқынды болуы және күнделікті қызметті шектеуі мүмкін.
Электр қыздырғыш жастықшасын қолдануға немесе жылы ванна қабылдап көруге болады. Сондай-ақ, етеккір алды синдромын бақылау үшін дәрілік препараттарды қабылдауға болады.
Бұл дәрілер аспириннің немесе ацетаминофеннің кофеинмен, антигистаминдік препараттармен немесе диуретиктермен бірігуі. Мысалы: Мидол, Памприн, Премзин ПМС.
Ауырсынуды басатын дәрілік препараттар да ауырсынуды жеңуге көмектеседі. Оларға жататандар: ибупрофен және напроксен. Бұл дәрілер жеңіл немесе орташа ауырсынуды басуға көмектеседі. Егер олар көмектеспейтін болса, дәрігермен күштірек препарат туралы кеңесіңіз.
Дәрігер ұрықтануға қарсы таблеткаларды тағайындауы мүмкін. Бұл дәрілер осы кезеңдердегі ауырсынуды жеңілдетеді.
Егер бұл әдістердің біреуі де көмектеспесе, дәрігер аналық бездің кистасының болуына немесе эндометриозға тексереді. Дәрігер УДТ (УЗИ) аналық бездің кистасының болуын көруге көмектеседі. Шағын оперативтік араласу – лапароскопия эндометриозды анықтау үшін қолданылады. Бұл әдіс теріде шағын тілік жасап, жіңішке түтік енгізу арқылы жатырдың ішін көруге мүмкіндік береді.
Іштің өтуі мен құсу қауіпті болуы мүмкін, себебі, организмнің сусыздануына апарады. Организм сұйықтықтың үлкен мөлшерін жоғалтқанда сусыздану дамиды. Егде жастағы адамдарда сусыздану тез дамиды, бірақ, сусыздану кез келген жаста пайда болуы мүмкін.
Құсу мен іштің өтуінің пайда болу себептері қандай?
Іштің өтуі мен құсу вирустық, бактериалдық, паразитарлық аурулардың симптомы, кейбір аурулар мен дәрілік препараттарды қабылдаудың салдары болуы мүмкін. Кейбір өнімдерді, шала піскен етті немесе балықты қорытудың бұзылысы да іштің өтуі мен құсуды туындатуы мүмкін.
Қалай организмнің сусыздануының алдын алуға болады?
Іштің өтуі мен құсу ұстамасы байқалған кез келген адамға жоғалтылған сұйықтық пен электролиттердің орнын толтыру қажет.
Іштің өтуі мен құсу кезінде жоғалтылған сұйықтықтың орнын толтыру үшін ересектер мен егде жастағы адамдар күніне, кемінде, 7-8 стақан су ішуі қажет. Егде адамдарға жоғалтылған сұйықтықтың орнын толтыру үшін ішуге арналған регидратациялау ерітінділері тағайындалуы мүмкін (нұсқау).
Құсу мен іштің өтуін тоқтату үшін дәрілік препараттарды қабылдау қажет пе?
Әдетте, қажеті жоқ, себебі, құсу мен іштің өтуі тез өтеді. Инфекциялар кезінде құсу мен іштің өтуі - инфекциялық бөлікті организмнен шығаруға организмнің қорғаныстық реакциясы. Құсу мен іштің өтуін тоқтататын дәрілерді қабылдау организмнің өздігінше қалпына келуіне кедергі келтіруі мүмкін. Сондай-ақ, антибиотиктерге де қажеттілік жоқ. Дәрілік препараттар қажет деп санасаңыз, дәрігерге айтыңыз.
Балаңызда немесе жақын адамыңызда сусыздану дамығандығын қалай білуге болады?
Адамда сусыздану дамығандығын болжау қиын. Әдетте, сусызданудың симптомдары ауыр дәрежесіне өткенде пайда болады. Сусызданудың келесі симптомдарының бірі байқалса, әсіресе, егде жастағы адамдарда, дәрігерге көріну қажет. Ауыр сусыздану жағдайында іштің өтуі мен құсу кезінде жоғалтылған сұйықтықтың орнын толтыру үшін науқасқа көктамыр (вена) арқылы сұйықтық енгізу қажет болуы мүмкін.
Сусызданудың симптомдары
Несептің мөлшерінің азаюы немесе болмауы, түсінің қошқыл болуы
Несептің жүруінің сиреуі
Шөлдеу
Ашушаңдық
Тәбеттің болмауы
Салмақ жоғалту
Ауыздың құрғауы
Терінің созылымдылығын және серпімділігін жоғалту
Ұйқы басуы.
Қашан дәрігерге көріну қажет
Іштің өтуі мен құсу ушығатын болса, немесе іштің өтуіне және/немесе құсуға ұшыраған адамда келесілер байқалса:
Сусыздану белгілері болса (жоғарыда келтірілген).
Құсу 8 сағаттан артық жалғасса немесе басылмайтын сипатта болса.
Нәжісте қан пайда болса.
Құсықта қан пайда болса.
8 сағат ішінде несептің жүруі болмаса.
Улы зат жұту кезінде.
Бұлшық еттің ширығуы немесе бастың күшті ауырсынуы болса.
Енжар немесе ұйқы басқан болса.
2 сағаттан артық уақыт бойы іште ауырсыну болса.
Дәрігерге қойылатын сұрақтар
Іштің өтуі мен құсу басқа аурудың симптомдары болуы мүмкін бе?
Іштің өтуі мен құсуды емдеу үшін қандай дәрілік препараттар көмектеседі?