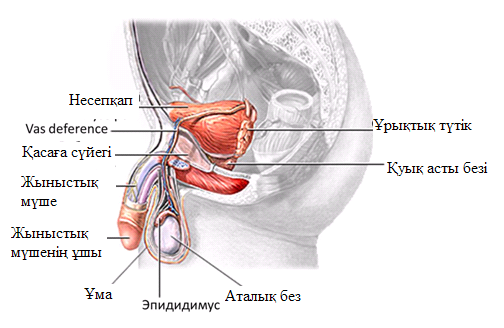
Шәуеттің жиналуы, жыныстық мүшенің күпегінің астында жағымсыз иісті қоймалжың заттектің жинақталуы жыныстық мүшенің қатерлі ісігінің даму қаупін арттырады.
Сүндетке отырғызылмаған, күпек аумағының тазалығын қадағаламайтын ерлер, сондай-ақ, үшкір кондилома немесе адам папиломасы вирусы (ВПЧ) бар ерлер осы сирек аурудың пайда болу қаупіне бейім келеді.
Дәрігер медициналық тексеруді өткізеді, оның барысында сыртқы пішіні безеу немесе сүйел секілді түзіліс анықталады. Бұл түзіліс, әдетте, пенистің ұшында орналасады.
Қатерлі ісік диагнозын қою үшін осы түзілістің биопсиясы жасалады.
Емдеу ісіктің өлшеміне және орналасуына, таралу ауданына байланысты.
Жалпы, қатерлі ісікті емдеуге кіретіндер:
Химиялық емдеу – қатерлі ісік жасушаларын жоятын дәрілік препараттарды қабылдау
Сәулелік емдеу – ісікті жою үшін күшті рентген сәулесі қолданылады.
Оперативтік емдеу – қатерлі ісікті хирургиялық жолмен алып тастау.
Егер ісік шағын болса, немесе жыныстық мүшенің ұшына жақын орналасса, пенистегі қатерлі ісік аумағын ғана алып тастау операциясы жасалады. Ісіктің нақты орналасуына сай операция глансэктомия немесе ішінара пенэктомия аталады. Кейбір ісіктерді емдеу үшін лазерлік операция қолданылуы мүмкін.
Күрделі ісіктер үшін жыныстық мүшені толық алып тастау қажет (жаппай пенэктомия). Бұл жағдайда организмнен несепті шығару үшін шаптың аумағында жаңа түтік жасалынады. Бұл шара уретростомия аталады.
Оперативтік араласумен қатар химиялық емдеу қолданылады. Әдетте, жыныстық мүшенің қатерлі ісігін емдеу үшін цисплатин, ифосфамид, паклитаксел тағайындалады.
Сәулелік емдеу, көбінесе, хирургиялық араласумен бірге ұсынылады. Мұндай жағдайда сыртқы сәулелік емдеу қолданылады. Бұл әдіс пенисті сыртынан сәулелендіруді қамтамасыз етеді. Сыртқы сәулелік емдеу аптасына 5 рет, 6-8 апта бойы жалғасады.
Ерте анықталып, емделсе, болжамы оң болуы мүмкін. Жыныстық мүшенің қатерлі ісігінде 5-жылдық тірі қалу 65% құрайды. Несеп шығару және жыныстық қызмет пенистің біршама бөлігін алып тастағанда да сақталуы мүмкін болады.
Сүндетке отырғызу қауіпті азайтады. Сүндетке отырғызылмаған ерлерге жасынан күпекті тазартуды түсіндіру қажет, бұл олардың жеке гигиенасының құраушысы.
Жеке гигенаны сақтау және қауіпсіз жыныстық қатынасты қолдау, жыныстық қатынаста серіктестердің санын шектеу, АИТВ инфекциясының алдын алу мақсатында презервативтер қолдану жыныстық мүшенің қатерлі ісігінің даму қаупін азайтады.
Аудармашы: Асель Стамбекова, HealthСity жобасының дербес үйлестірушісі
Редакциялық алқа:
Алмаз Шарман, медицина профессоры
Ләзат Ақтаева, м.ғ.д.
Сәлім Смайылов, б.ғ.к.
Материал подготовлен профессором медицины Алмазом Шарманом на основании публикации Национального института онкологии США «Что вам нужно знать о раке матки» (What do you need to know about uterine cancer).
МАТКА
Матка является частью репродуктивной системы женщины. Она представляет собой полый орган грушевидной формы, в котором происходит развитие плода. Матка расположена в малом тазу между мочевым пузырем и прямой кишкой. Матка имеет шейку, которая представляет собой сужение, расположенной в нижней части матки. Широкая часть матки, расположенная выше шейки, называется телом матки. Куполообразная верхняя часть органа называется дном матки. Фаллопиевы трубы представляют собой отростки матки, расположенные по обе стороны органа. Они заканчиваются яичниками.
Стенка матки состоит из двух слоев. Внутренний слой называется эндометрием. Наружный слой стенки матки представлен мышечной тканью и называется миометрием. У женщин детородного возраста каждый месяц происходит утолщение эндометрия, что связано с подготовкой матки к беременности. Если беременность не наступает, толстый внешний слой эндометрия отторгается и выходит через влагалище вместе с кровяными массами. Это явление называется менструацией.
ЧТО ТАКОЕ РАК?
Рак начинается в клетках, строительных элементах, формирующих ткани. Ткани образуют органы. В норме клетки растут и делятся, образуя новые клетки, по мере того, как организм в них нуждается. Старея, клетки погибают, и их место занимают новые клетки. Иногда этот упорядоченный процесс нарушается. Новые клетки образуются тогда, когда они не нужны организму, а старые клетки не погибают вовремя. Эти дополнительные клетки образуют массу ткани, называемую новообразованием или опухолью.
Опухоли бывают доброкачественными и злокачественными: Доброкачественные опухоли не относятся к категории раковых.
· Доброкачественные опухоли редко угрожают жизни.
· Обычно доброкачественные опухоли удаляются и не вырастают вновь.
· Клетки доброкачественных опухолей не прорастают в окружающие их ткани.
· Клетки доброкачественных опухолей не распространяются на другие органы и части тела. Доброкачественными опухолями матки являются следующие: Фиброидные опухоли (миома матки) - являются распространенными опухолями, произрастающими из мышечного слоя матки. Они чаще всего возникают у женщин после сорока лет. Женщины с такой опухолью могут одновременно иметь несколько фиброидных узлов. Фиброидная опухоль не переходит в рак. При переходе в менопаузу фиброидная опухоль чаще всего уменьшается в размерах и может сама по себе исчезнуть. Обычно фиброидные опухоли (миома матки) не вызывают никаких симптомов. Однако в зависимости от размеров и локализации фиброидные узлы могут сопровождаться кровотечениями, выделениями из влагалища и частыми мочеиспусканиями. Женщинам с такими симптомами рекомендуется обратиться к врачу. Если наблюдается сильное кровотечение или, когда опухоль давит на близлежащие органы, вызывая болезненные ощущения, врач может рекомендовать хирургическое вмешательство или другие виды лечения.
Эндометриоз представляет собой другой вид доброкачественных изменений матки. Он чаще всего наблюдается у женщин в возрасте 30 – 40 лет, особенно у тех, у кого никогда не наступала беременность. Эндометриоз характеризуется разрастанием эндометриальной ткани за пределы матки с распространением на близлежащие органы. При этом могут наблюдаться болезненные менструации, патологические выделения из влагалища и иногда бесплодие. Однако эндометриоз не вызывает рак матки. Женщинам с эндометриозом обычно рекомендуют так называемую гормональную терапию.
Гиперплазия эндометрия – это другое доброкачественное состояние, характеризующееся увеличением числа клеток во внутреннем слое матки. Гиперплазия эндометрия – это не рак, однако это состояние может перейти в рак. Гиперплазия эндометрия характеризуется усилением менструаций, кровотечением в период между менструациями, а также выделениями крови в период менопаузы. Данное состояние чаще всего наблюдается у женщин после 40 лет.
Для того чтобы предупредить развитие рака врач может рекомендовать удаление матки (гистерэктомию) у женщины с гиперплазией эндометрия. Также можно рекомендовать лечение с помощью гормонов (прогестерон) и постоянное наблюдение у гинеколога.
Злокачественные опухоли являются раковыми:
· Злокачественные опухоли чаще всего имеют более серьезные симптомы, чем доброкачественные. Они могут нести угрозу жизни пациента.
· Злокачественные опухоли во многих случаях могут быть удалены, но иногда вырастают снова.
· Клетки злокачественных опухолей могут прорастать и повреждать прилежащие ткани и органы.
· Клетки из злокачественных опухолей могут распространяться (метастазировать) в другие органы и части тела. Раковые клетки распространяются посредством попадания отсоединившихся частей первоначальной опухоли в кровоток или в лимфатическую систему. Клетки могут прорастать в другие органы, образуя новые опухоли, которые повреждают эти органы. Раковые клетки, распространяющиеся по другим органам, называются местастазами, а процесс распространения – метастазированием. Распространение рака матки (метастазирование) характеризуется обнаружением раковых клеток в близлежащих лимфатических узлах, нервной ткани и кровеносных сосудах. Метастазы в близлежащие лимфоузлы могут далее распространяться в удаленные лимфоузлы и другие органы, такие как легкие, печень и кости.
При распространении рака и образовании новой опухоли в другом органе или части тела, новая опухоль состоит из тех же аномальных клеток и носит то же название, что и первоначальная. Например, если рак матки распространился в легкие, раковые клетки, обнаруживаемые в легких - это раковые клетки матки. Заболевание представляет собой метастатический рак матки, а не рак легких. По этой причине он лечится как рак матки, а не как рак легких. Врачи иногда называют новую опухоль «дистантной» или метастатической болезнью.
Рак матки чаще всего развивается из внутреннего слоя – эндометрия. Такой вид рака называется эндометриальным раком, однако, чаще всего применяют название рака матки, подразумевая при этом, что рак начался из эндометрия.
СИМПТОМЫ РАКА МАТКИ
Рак матки чаще всего развивается после менопаузы. Однако он может развиться и во время менопаузы. Патологические кровянистые выделения из влагалища является наиболее распространенным симптомом рака матки. Кровотечение может начинаться в виде водянистых выделений с небольшим количеством крови, которые становятся все более кровянистыми. Это немедленно должно вызывать подозрение, поскольку кровотечение не является признаком менопаузы.
Женщине необходимо обратиться к врачу, если у нее возник, по меньшей мере, один из следующих симптомов:
· Необычные выделения или кровотечения из влагалища
· Затрудненное или болезненное мочеиспускание
· Болезненные ощущения во время полового контакта
· Боль в малом тазуУказанные симптомы могут быть вызваны раковым процессом или другими серьезными проблемами. Чаще всего они не связаны с раком, однако только врач может поставить достоверный диагноз.
ДИАГНОСТИКА РАКА МАТКИ
Если у женщины возникли симптомы, вызывающие подозрение на рак матки, ей рекомендуется обратиться к врачу, который проведет общее обследование и направит кровь и мочу на анализы. Врач может посчитать необходимым проведение следующих видов обследования:
· Гинекологическое исследование – врач проводит исследование органов малого таза – влагалища, матки, мочевого пузыря и прямой кишки. Исследование проводится для изучения размеров и структуры указанных органов. Исследование влагалища и шейки матки может проводиться с помощью специальных приборов.
· Мазок из шейки матки – врач собирает мазок из шейки матки и верхней части влагалища для лабораторного исследования и микроскопического выявления патологических клеток. Этот тест также носит название мазка по Папаниколау (по имени автора) или Пап-теста. Хотя данный тест позволяет установить раковые клетки в шейке матки, для выявления рака самой матки необходимо провести биопсию, то есть завести специальный инструмент в полость матки и захватить кусочек ткани для микроскопического изучения.
· Трансвагинальное ультразвуковое исследование – Врач вводит специальный инструмент во влагалище, который с помощью отражения высокочастотных волн позволяет рассмотреть структуру внутренней поверхности матки. В частности, данный метод позволяет выявить патологическое утолщение эндометрия, что является основание для проведения биопсии.
· Биопсия – врач забирает кусочек ткани из внутренней поверхности матки. Эта процедуру проводится путем введения в матку специального инструмента, что может потребовать расширения шейки матки. Одновременно можно провести выскабливание слизистой оболочки матки для изучения ее содержимого. Далее проводится микроскопическое исследование ткани, полученной с помощью биопсии, а также материалов выскабливания для выявления гиперплазии или наличия раковых клеток и другой патологии. В течение определенного времени после такой процедуры женщина может чувствовать неприятные ощущения в нижней части живота и небольшие кровянистые выделения.
СТАДИИ РАЗВИТИЯ РАКА МАТКИ
После установления диагноза врач должен знать, на какой стадии находится раковый процесс с тем, чтобы назначить правильное лечение. Выяснение стадии заболевания является попыткой выяснить в какой степени распространился рак, и на какие органы произошло распространение.
Для выяснения данного вопроса врач может назначить исследования крови и мочи, а также рентгенологическое исследование. Кроме того, может оказаться необходимым проведение компьютерной томографии, ультразвукового исследования, ядерно-магнитного резонанса, сигмоидоскопии или колоноскопии.
В большинстве случаев наиболее достоверным путем выяснения стадии рака является удаление матки (гистерэктомия) и установление степени распространения ракового процесса визуальным путем, то есть невооруженным глазом. В частности, важным является выяснение того, поражена ли мышечная ткань матки, и произошло ли распространение на лимфатические узлы и близлежащие органы малого таза. Также проводится микроскопическое исследование полученной ткани на наличие раковых клеток.
Стадийность рака матки устанавливается на основе следующих признаков:
· Стадия I – Раковый процесс поражает только тело матки и не распространяется на шейку.
· Стадия II – Раковый процесс распространился от тела матки на шейку.
· Стадия III – Раковый процесс распространился за пределы матки, но не вышел за пределы малого таза (однако пока не поразил мочевой пузырь и прямую кишку). Лимфатические узлы малого таза содержат раковые клетки.
· Стадия IV – Раковый процесс распространился на мочевой пузырь и прямую кишку или он распространился за пределы малого таза на другие органы.
ЛЕЧЕНИЕ РАКА МАТКИ
Многие женщины, которым поставлен диагноз «Рак матки» хотят принимать активное участие в принятии решения о необходимости и методах лечения. Однако состояние шока и стресса из-за поставленного диагноза затрудняет адекватное восприятие болезни и, зачастую больные забывают многие вопросы, которые они хотели бы задать врачу. По указанной причине на прием к врачу лучше приходить с родственником или другом, который может помочь больному.
Врач может направить больного к специалисту, например к гинекологу (специалисту, который лечит женские болезни), или к онкологу (специалисту, который лечит раковые болезни).
Методы лечения Выбор методов лечения рака матки зависит от размеров опухоли, стадии заболевания, а также от того, в какой степени женские гормоны влияют на рост опухоли. Важным фактором также является степень дифференциации раковых клеток, то есть, то в какой степени они отличаются от нормальных клеток. Чем больше отличие, тем быстрее рост опухоли. Кроме того, фактором в принятии решения о методах лечения является общее состояние здоровья женщины.
Существует ряд методов лечения рака матки. Большинству женщин с раком матки проводят хирургическое лечение. Некоторым назначают радиационную терапию. Иногда рекомендуется так называемая гормональная терапия. Некоторым больным назначают комбинированное лечение.
Большинству женщин с раком матки положено хирургическое вмешательство с целью удаления матки - гистерэктомии. Операцию проводят путем надреза на брюшной стенке. Хирург обычно вместе с маткой удаляет обе фаллопиевы трубы и яичники, то есть проводит так называемую билатеральную сальпинго-оофоректомию.
Хирург также может удалить лимфатические узлы, если они содержат раковые клетки. Если раковые клетки обнаруживаются в лимфатических узлах, это означает, что раковый процесс распространился на другие части организма. Если рак ограничился эндометрием, женщине может и не потребоваться дополнительных методов лечения, кроме хирургической операции.
Радиационная терапия характеризуется использованием радиоактивных лучей с высокой энергией, которые способны уничтожать раковые клетки. Аналогично хирургическому вмешательству, радиотерапия относится к местным видам лечения, поскольку она уничтожает раковые клетки только в зоне воздействия.
Некоторые женщины с раком матки на стадиях I, II или III нуждаются в комбинации хирургического вмешательства с радиационной терапией. Им могут вначале провести радиотерапию для уменьшения размеров опухоли, а затем хирургическую операцию. Однако чаще всего радиотерапию проводят после хирургической операции для того, чтобы уничтожить оставшуюся опухоль. Кроме того, радиотерапию назначают некоторым женщинам, которым не показана хирургическая операция.
Для лечения рака матки используют два типа радиационной терапии:
· Внешняя радиотерапия: для внешней радиотерапии используют внешний источник радиации (специальный аппарат), лучи которого направляют на место локализации опухоли. Такое лечение проводят 5 дней в неделю в течение нескольких недель. Это позволяет фокусированно влиять на раковые клетки.
· Внутренняя радиация: для внутренней радиотерапии через влагалище вводят (имплантируют) специальную маленькую радиационную трубку и оставляют ее на несколько дней. На период лечение рекомендуют ограничить контакт женщины с родственниками и друзьями. После удаления такой трубки общение становится вполне безопасным. Для некоторых женщин показана комбинация как внешней, так и внутренней радиотерапии.
Гормональная терапия предусматривает использование специальных средств, препятствующих раковым клеткам контактировать с гормонами, которые стимулирую рост опухоли. Гормоны взаимодействуют с раковыми клетками посредством специальных рецепторов. До начала гормональной терапии проводят тестирование на гормональные рецепторы, а именно на наличие в матке эстрогеновых и прогестероновых рецепторов. Если рецепторы присутствуют, то высока вероятность того, что раковая опухоль отреагирует на гормональную терапию.
Гормональная терапия относится к категории системной терапии, поскольку она влияет на раковые клетки по всему организму. Обычно в качестве гормональной терапии применяют таблетки, содержащие прогестерон. Иногда гормональную терапию проводят женщинам, которым противопоказано хирургическое вмешательство или радиотерапия. Кроме того, врач может назначить гормональную терапию больным, у которых опухоль распространилась на легкие и другие отдаленные органы. Также гормональную терапию назначают женщинам с повторным раком матки.
ПОБОЧНЫЕ ЭФФЕКТЫ ЛЕЧЕНИЯ РАКА МАТКИ
Побочные эффекты хирургического лечения После гистеректомии у женщин отмечается слабость и болезненные ощущения. У большинства женщин восстановление происходит на 4 – 8 неделе. Однако многим женщинам потребуется больше времени, чтобы восстановиться. Некоторые больные жалуются на тошноту и рвоту после оперативного вмешательства. Также могут отмечаться проблемы с мочевым пузырем и кишечником. Врач рекомендует ограничить на некоторое время прием пищи и жидкости. Постепенно женщина возвращается к нормальному питанию.
После гистеректомии у женщины исчезают менструации, и она больше никогда не сможет забеременеть. Проявления климакса у таких женщин обычно бывают более выраженными. В таких случаях иногда рекомендуют так называемую заместительную терапию в виде эстроген-содержащих препаратов. Они позволяют облегчить состояние. Однако некоторые врачи придерживаются мнения, что больным, у которых когда-либо был рак матки, не следует давать эстроген. После гистеректомии у многих женщин нарушается сексуальная функция в виде уменьшения полового влечения. О такой возможности необходимо сообщить мужу/партнеру.
Побочные эффекты радиационной терапии Побочные эффекты радиационной терапии в основном зависят от применяемой дозы и места воздействия радиоактивных лучей. Распространенными побочными эффектами являются сухость и покраснение кожи в месте воздействия, потеря аппетита и слабость. Некоторые женщины жалуются на ощущения сухости, зуд и жжение во влагалище. Кроме того, радиация может вызывать диарею, а также частое и болезненное мочеиспускание. Результатом воздействия радиации также является уменьшение числа белых кровяных клеток (лейкоцитов), которые призваны защищать от инфекции. Врач рекомендует женщинам, подвергающимся радиационной терапии, не вступать в половые контакты. Однако спустя несколько недель после радиационной терапии, женщина может возобновить половые связи.
Побочные эффекты гормональной терапии Организм женщины, принимающей таблетки с прогестероном, склонен задерживать жидкости. Также побочным эффектом гормональной терапии является повышение аппетита и прибавка в весе. У женщин с сохраненной менструальной функцией могут происходить нарушения менструации.
ДОПОЛНИТЕЛЬНАЯ И АЛЬТЕРНАТИВНАЯ ТЕРАПИЯ
Некоторые больные раком предпочитают методы дополнительной и альтернативной медицины: К дополнительным методам относятся те, которые применяются наряду со стандартными методами лечения рака, такими как химиотерапия и радиотерапия. Альтернативные методы – это те, которые применяется вместо стандартных методов лечения.
Акупунктура (иглотерапия), лечебный массаж, производные трав, витамины или специальные диеты, визуализация, медитация и духовное лечение относятся к разновидностям дополнительной или альтернативной медицины. Некоторые онкологические больные отмечают улучшение самочувствия в результате применения методов дополнительной или альтернативной терапии. Следует учитывать, однако, что некоторые виды дополнительной и альтернативной медицины могут изменить механизмы воздействия химиотерапии и радиотерапии. Эти изменения могут нанести вред больному. Кроме того, некоторые виды дополнительной и альтернативной медицины сами по себе могут оказаться вредными, даже если применяются отдельно. Некоторые виды дополнительной и альтернативной медицины являются дорогостоящими.
ПОДДЕРЖКА И УХОД ЗА БОЛЬНЫМИ
Жить с таким серьезным заболеванием, как рак, нелегко. Некоторым людям бывает нужна помощь в решении эмоциональных и практических проблем, связанных с их заболеванием. В таких случаях весьма полезными могут оказаться группы взаимоподдержки. Данная концепция получила распространения в ряде западных стран. В таких группах больные раком собираются, чтобы поделиться своими знаниями и опытом в том, как справляться с болезнью и последствиями лечения.
Онкологические больные часто беспокоятся о своих семьях, о сохранении своих рабочих мест, о сохранении ежедневной жизнедеятельности. Обеспокоенность необходимостью обследований, лечения, госпитализации, а также стоимость медицинских услуг также характерны для таких больных. На многие вопросы, беспокоящие онкологических больных, обычно отвечают медработники.
ПИТАНИЕ И ФИЗИЧЕСКАЯ АКТИВНОСТЬ
Для онкологических больных очень важно следить за собой. Это подразумевает хорошее питание и поддержание максимально возможной активности. Онкологическим больным необходимо получать достаточное количество калорий для поддержания хорошего веса. В частности, необходимо получать достаточное количество белка. Хорошее питание помогает улучшить самочувствие и получать больше энергии.
Часто у онкологических больных, особенно во время или сразу после лечения может снизиться аппетит. Они могут почувствовать недомогание или усталость, или изменение вкусовых ощущений. Кроме того, побочные эффекты лечения (такие как плохой аппетит, тошнота, рвота или болячки во рту) могут вызывать серьезную проблему. Врач, диетолог или другой медицинский сотрудник могут предложить способы решения проблем с питанием.
Многие люди чувствуют себя лучше, сохраняя активный образ жизни. Ходьба, занятия йогой, плавание и другие виды занятий помогают оставаться сильными и сохранять энергию и жизненный тонус. Упражнения помогают уменьшить тошноту и боль и тем самым облегчить процесс лечения. Они также способствуют освобождению от стресса. Очень важно проконсультироваться у врача относительно вида физической нагрузки. Если физические упражнения вызывают боль или другие проблемы, необходимо сообщить об этом врачу для того, чтобы решить вопрос об изменении характера физической нагрузки.
ПОСЛЕДУЮЩЕЕ НАБЛЮДЕНИЕ
Наблюдение за больным после лечения является исключительно важным. Врач должен наблюдать за состоянием больной, чтобы не упустить начала возобновления ракового процесса. Периодические осмотры позволяют установить такие изменения. Для этого необходимо периодически проводить гинекологические обследования, лабораторные тесты, рентгенологические исследования и др.
НАУЧНЫЕ РАЗРАБОТКИ
В настоящее время ученые разрабатывают методы щадящих хирургических вмешательств по удалению матки. В частности, разрабатываются методы удаления матки с помощью лапароскопа, который вводят через влагалище. Таким образом возможно избежать обширного разреза на брюшной стенке и провести щадящее исследование брюшной полости на предмет распространения рака.
Другие группы исследователей изучают пути эффективного использования радиационной терапии после хирургических вмешательств, а также применение комбинированного применения хирургии, химиотерапии и радиотерапии. В США и других странах проводят клинические испытания новых лекарств и их комбинаций, а также методов биологической терапии. Некоторые из этих исследований направлены на изучение путей снижения побочных эффектов и улучшение качества жизни больных.
What is endometrial cancer and what should I watch for?
Endometrial cancer is cancer of the endometrium. The endometrium is the lining of the uterus (sometimes called the womb). Endometrial cancer can almost always be treated successfully if it's caught early. You can increase the chances that endometrial cancer will be found early by telling your doctor about any unusual bleeding.
What are the symptoms of endometrial cancer?
The most common sign of endometrial cancer is unusual bleeding from your vagina, especially bleeding after menopause.
Am I at risk for endometrial cancer?
Certain things may put you at greater risk for getting endometrial cancer. One risk factor is age. Endometrial cancer is most common in women who are older than 50 years of age.
You may also be at greater risk if you have had high levels of estrogen in your body. Many things can increase your estrogen level. These include being extremely overweight, having high blood pressure or having diabetes.
Using estrogen replacement therapy without taking progestin may also increase the risk for endometrial cancer. For this reason, women who use hormone replacement therapy (HRT) usually take a combination of estrogen and the hormone progestin. While estrogen stimulates growth of the endometrium, progestin seems to protect the lining of the uterus from the estrogen. In fact, using birth control pills that contain both estrogen and progestin during the childbearing years seems to decrease a woman's risk of endometrial cancer.
Other things that may put you at greater risk for endometrial cancer include having your first period before 12 years of age or going through menopause after 50 years of age. Women who have never been pregnant and women who use a medicine called tamoxifen may also be at greater risk.
How is endometrial cancer diagnosed?
Your doctor will diagnose endometrial cancer by performing one or more of the following procedures:
· Endometrial biopsy is usually done in your doctor’s office. It involves inserting a narrow tube into the uterus through the vagina and removing a small amount of tissue from the uterine wall. This tissue is tested in a lab for cancerous or precancerous cells. The procedure usually takes just a few minutes.
· Dilatation and curettage (D & C) involves dilating (widening) the cervix (the opening of the uterus) and inserting an instrument to scrape or suction the uterine wall and collect tissue. D & C is also an outpatient procedure. It takes about an hour and usually requires general anesthesia (puts you in a sleep-like state).
· Imaging tests are used in patients who have certain medical conditions such as severe high blood pressure, obesity, diabetes, or other types of cancer. These patients may not be able to safely have anesthesia. In these patients, imaging tests such as an MRI scan, CT scan, or ultrasound may help diagnose cancer of the uterus.
Your doctor will talk to you about which procedure is right for you.
What is the treatment for endometrial cancer?
Treatment usually involves removing the uterus, the fallopian tubes and the ovaries. You may also need to take progestin to balance out high levels of estrogen. Sometimes radiation therapy or chemotherapy is also needed. Treatment can be very effective, especially if the cancer is found early.
Questions to Ask Your Doctor
· I’ve gone through menopause and I’m still bleeding. Could I have endometrial cancer?
· I have endometrial cancer. Is there a higher risk that my daughter could get it, too?
· Will I have to have a hysterectomy?
· If I have a hysterectomy, will I have to take hormones afterward?
· How long will my treatment last?
· I once took tamoxifen for breast cancer. Should I be tested for endometrial cancer on a regular basis?
· How often after my treatment ends will I have to come in to see the doctor for follow-up exams?
· What are some of the side effects of hysterectomy?
Skin cancer is the most common form of cancer. Fortunately, it is usually one of the most curable types of cancer.
The body is made up of many types of cells. Normally, cells grow, divide and die. Sometimes, cells mutate (change) and begin to grow and divide more quickly than normal cells. Instead of dying, these abnormal cells clump together to form tumors. If these tumors are cancerous (also called "malignant"), they can invade and kill your body's healthy tissues. From these tumors, cancer cells can metastasize (spread) and form new tumors in other parts of the body. By contrast, noncancerous tumors (also called "benign") do not spread to other parts of the body.
More than 1 million people will be diagnosed with skin cancer this year. Almost all skin cancers are the result of too much exposure to ultraviolet light, which is found in sunlight and in lights used in tanning salons.
What is melanoma?
There are 2 forms of skin cancer: melanoma (the less common but more serious kind) and nonmelanoma (the more common, very treatable type). Most skin cancers don’t spread, but melanoma is very serious. It can spread through the whole body. If it is found early, it can be cured. If it is found late, it may cause death.
On what parts of the body is skin cancer most likely to occur?
Most skin cancers occur on parts of the body that are repeatedly exposed to the sun. These areas include the head, neck, face, tips of the ears, hands, forearms, shoulders, back, chests of men, and the back and lower legs of women.
Melanomas can be anywhere on your body. In men, they are most often on the chest, stomach or back. In women, they are most often on the lower legs.
What does skin cancer look like?
Skin cancer can look different, depending on the type and location of the cancer. It's important to find skin cancer as early as possible. The best way to do this is to keep an eye on your skin, especially moles. Check your skin often and see your doctor if you notice any new bumps, growths, lesions, or rough patches of skin, or if you have new or suspicious looking moles.
A normal mole is solid tan, brown, dark brown or flesh colored. Its edges are well-defined. It's usually smaller than 1/4 inch in diameter and has a round or oval shape. It should be flat or dome-like.
The ABCDE rule can help you remember what to look for when you're checking moles on your skin. If you notice any of these signs, talk to your doctor right away.
Signs of skin cancer: The ABCDE rule
A for asymmetry: A mole that, when divided in half, doesn't look the same on both sides.
B for border: A mole with edges that are blurry or jagged.
C for color: Changes in the color of a mole, including darkening, spread of color, loss of color, or the appearance of multiple colors such as blue, red, white, pink, purple or gray.
D for diameter: A mole larger than 1/4 inch in diameter (about the size of a pencil eraser).
E for elevation: A mole that is raised above the skin and has an uneven surface.
What are some other signs of skin cancer?
Other signs of skin cancer may include the following:
A mole that bleeds
A fast-growing mole
A scaly or crusted growth on the skin
A sore that won't heal
A mole that itches
A new mole that appears after you are 30 years of age.
A place on your skin that feels rough, like sandpaper
Patches of skin that have changed color, including brown, red, white, blue, or black
Also be aware that moles can grow in hidden areas of your body, such as between toes, on your scalp or under a nail. If you notice a mole that has changed, or if you have a new mole that doesn't look like your other moles, visit your doctor right away.
Why is the sun so bad for my skin?
The sun's rays, which are called ultraviolet A and ultraviolet B rays (UVA and UVB rays) damage your skin. This leads to early wrinkles, skin cancer and other skin problems.
Being in the sun too often for too long can lead to skin cancer, even if you don't burn. A tan is the body's attempt to protect itself from the sun's harmful rays.
Are tanning booths safer?
No. Tanning booths use ultraviolet rays. Makers of the booths may claim that they use "harmless" UVA rays. But both UVA and UVB rays cause skin damage. While UVA rays take longer than UVB rays to damage the skin, they go deeper into the skin than UVB rays.
What are the risk factors for skin cancer?
A number of factors may put you at higher risk of having skin cancer, including the following:
Having fair skin and red or blond hair
Having light-colored eyes
Sunburning easily
Having many moles, freckles or birthmarks
Working or playing outside
Being in the sun a lot as a child
Having had a serious sunburn
Having had skin cancer, or having family members who have had skin cancer
Tanning in the sun or with a sunlamp
Who gets melanoma?
Anyone can get melanoma, but some people are more likely to get it. If you answer "yes" to any of the questions below, you may be more at risk. Talk with your doctor about your risk factors.
Has anyone in your family had cancerous moles or a melanoma?
Do you have many moles larger than a pencil eraser?
Do you have more than 50 moles of any size?
Did you ever get a bad sunburn that caused blisters when you were a child?
Does your skin usually burn but not tan?
What's the best way to do a skin self-examination?
The best way is to use a full-length mirror and a hand-held mirror to check every inch of your skin.
1. First, you need to learn where your birthmarks, moles and blemishes are and what they usually look like. Check for anything new, such as a change in the size, texture or color of a mole, or a sore that doesn't heal.
2. Look at the front and back of your body in the mirror, then raise your arms and look at the left and right sides.
3. Bend your elbows and look carefully at your palms and forearms, including the undersides, and your upper arms.
4. Check the back and front of your legs.
5. Look between your buttocks and around your genital area.
6. Sit and closely examine your feet, including the bottoms of your feet and the spaces between your toes.
7. Look at your face, neck and scalp. You may want to use a comb or a blow dryer to move hair so that you can see better.
By checking yourself regularly, you'll get familiar with what's normal for you. If you find anything unusual, see your doctor. The earlier skin cancer is found, the better.
How will my doctor diagnose skin cancer?
Your doctor will examine your skin. If you have skin changes that might be skin cancer, your doctor will do a biopsy. During a biopsy, a small piece of your skin is removed and sent to the lab for testing.
Treatment
What's the best way to do a skin self-examination?
The best way is to use a full-length mirror and a hand-held mirror to check every inch of your skin.
1. First, you need to learn where your birthmarks, moles and blemishes are and what they usually look like. Check for anything new, such as a change in the size, texture or color of a mole, or a sore that doesn't heal.
2. Look at the front and back of your body in the mirror, then raise your arms and look at the left and right sides.
3. Bend your elbows and look carefully at your palms and forearms, including the undersides, and your upper arms.
4. Check the back and front of your legs.
5. Look between your buttocks and around your genital area.
6. Sit and closely examine your feet, including the bottoms of your feet and the spaces between your toes.
7. Look at your face, neck and scalp. You may want to use a comb or a blow dryer to move hair so that you can see better.
By checking yourself regularly, you'll get familiar with what's normal for you. If you find anything unusual, see your doctor. The earlier skin cancer is found, the better.
How will my doctor diagnose skin cancer?
Your doctor will examine your skin. If you have skin changes that might be skin cancer, your doctor will do a biopsy. During a biopsy, a small piece of your skin is removed and sent to the lab for testing.
How can I prevent skin cancer?
The key is to avoid being in the sun or using sunlamps. If you're going to be in the sun for any length of time, follow the safe-sun guidelines.
Remember that clouds and water won't protect you—60% to 80% of the sun's rays go through clouds and can reach swimmers at least one foot below the surface of the water. The sun's rays can also reflect off water, snow and white sand.
What are the safe-sun guidelines?
Safe-sun guidelines are the following 4 ways to protect your skin and reduce your risk of skin cancer. Each is just part of a program to prevent skin cancer. To greatly lower your risk, you must follow all of the safe-sun guidelines.
1. Avoid the sun.
Sunlight damages your skin. The sun is strongest during the middle of the day, between 10 a.m. and 4 p.m. During these hours, the sun can do the most damage to your skin. Sunburns and suntans are signs that your skin has been damaged. The more damage the sun does to your skin, the more likely you are to get early wrinkles, skin cancer and other skin problems.
2. Use sunscreen.
Use a sunscreen or sunblock with a sun protection factor (SPF) of at least 15, even on cloudy days. Check the expiration date—some ingredients in sunscreen break down over time. Use plenty of sunscreen and rub it in well. You should put the sunscreen on 30 minutes before you go into the sun. Put the sunscreen everywhere the sun's rays might touch you, including your ears, the back of your neck and any bald areas on the top of the head. Be sure to apply enough sunscreen to cover all skin that may be exposed to the sun. Put on more sunscreen every hour or so if you're sweating or swimming. If you are using a sunscreen spray lotion, keep the spray bottle close to the part the body you are spraying. If you spray from too far away, you may not cover all skin that the sun’s rays will touch.
But don't think that you're completely safe from the sun just because you're wearing sunscreen. Sunscreen cannot give you 100% protection against the sun's harmful UV radiation.
3. Wear a wide-brimmed hat, protective clothing and sunglasses.
If you have to be out in the sun, cover up your skin. A wide-brimmed hat will help protect your face, neck and ears from the sun. A hat with a 6-inch brim all around is the best. Baseball caps don't protect the back of your neck or the tops of your ears. Wear sunglasses to protect your eyes from the sun. Choose sunglasses that block both ultraviolet-A (UVA) and ultraviolet-B (UVB) rays; wear sunglasses that wrap and are rated to block at least 99% of UVA sunlight. Sun exposure increases your risk of getting cataracts.
Wear protective clothing, such as long-sleeved shirts and long pants made of tightly woven fabric. If the clothes fit loosely, you will feel cooler. Special sun-protective clothes are available from several companies.
Remember that you are often exposed to the sun while driving, especially your hands and arms.
4. Don't try to get a tan.
Don't use tanning salons or sunlamps. Tanning booths and sunlamps damage your skin just like real sunlight does.
What else should I do?
Some doctors think it's a good idea to do a monthly skin check, especially if you are someone with risk factors for melanoma. Ask your doctor about this. If your doctor thinks it's a good idea for you, check your skin once a month for signs of skin cancer, such as irregular moles. The earlier skin cancer is found, the greater the chance that it can be cured. Try doing your skin check on the same date every month. Pick a day that you can remember, like the date of your birthday or the day you pay bills. Look for any changes in a mole or the appearance of a new mole. Any moles that appear after you turn 30 years of age should be watched carefully and shown to your doctor.
Sunburns in childhood are the most damaging. Children younger than 6 months of age should never be outside in direct sunshine. Children 6 months of age or older should wear sunscreen every day.
Questions to Ask Your Doctor
I have a mole that’s getting bigger. Could it be skin cancer?
I spent a lot of time in the sun as a child. Should I be checked for skin cancer regularly?
My father had skin cancer. Am I more likely to have it, too?
What is the best way to protect my child from the sun?
I like to swim. Will the water protect me from the sun?
A primary brain tumor is a group (mass) of abnormal cells that start in the brain.
Causes
Primary brain tumors include any tumor that starts in the brain. Primary brain tumors can start from brain cells, the membranes around the brain (meninges), nerves, or glands.
Tumors can directly destroy brain cells. They can also damage cells by producing inflammation, placing pressure on other parts of the brain, and increasing pressure within the skull.
The cause of primary brain tumors is unknown. There are many risk factors that could play a role:
Radiation therapy used to treat brain cancers increases the risk of brain tumors up to 20 or 30 years later.
Some inherited conditions increase the risk of brain tumors, including neurofibromatosis, Von Hippel-Lindau syndrome, Li-Fraumeni syndrome, and Turcot syndrome.
Lymphomas that begin in the brain in people with a weakened immune system are sometimes linked to infection by the Epstein-Barr virus.
Exposure to radiation at work or to power lines, as well as head injuries, smoking, and hormone therapy have not been proven to be risk factors.
Studies have found that cell phones, cordless phones, and wireless devices are safe and do not increase the risk.
Specific tumor types
Brain tumors are classified depending on:
Location of the tumor
Type of tissue involved
Whether they are noncancerous (benign) or cancerous (malignant)
Other factors
Sometimes, tumors that start out less aggressive can change their biologic behavior and become more aggressive.
Tumors can occur at any age, but many types are most common in a certain age group. In adults, gliomas and meningiomas are the most common.
Gliomas come from glial cells such as astrocytes, oligodendrocytes, and ependymal cells. Gliomas are divided into three types:
Astrocytic tumors include astrocytomas (can be noncancerous), anaplastic astrocytomas, and glioblastomas.
Oligodendroglial tumors. Some primary brain tumors are made up of both astrocytic and oligodendrocytic tumors. These are called mixed gliomas.
Glioblastomas are the most aggressive type of primary brain tumor.
Meningiomas and schwannomas are two other types of brain tumors. These tumors:
Occur most often between ages 40 and 70.
Are usually noncancerous, but can still cause serious complications and death from their size or location. Some are cancerous and aggressive.
Other primary brain tumors in adults are rare. These include:
Ependymomas
Craniopharyngiomas
Pituitary tumors
Primary (central nervous system - CNS) lymphoma
Pineal gland tumors
Primary germ cell tumors of the brain
Symptoms
Some tumors do not cause symptoms until they are very large. Other tumors have symptoms that develop slowly.
Symptoms depend on the tumor's size, location, how far it has spread, and whether there is brain swelling. The most common symptoms are:
Be worse when the person wakes up in the morning, and clear up in a few hours
Occur during sleep
Occur with vomiting, confusion, double vision, weakness, or numbness
Get worse with coughing or exercise, or with a change in body position
Other symptoms can include:
Change in alertness (including sleepiness, unconsciousness, and coma)
Changes in hearing, taste, or smell
Changes that affect touch and the ability to feel pain, pressure, different temperatures, or other stimuli
Confusion or memory loss
Difficulty swallowing
Difficulty writing or reading
Dizziness or abnormal sensation of movement (vertigo)
Eye problems such as eyelid drooping, pupils of different sizes, uncontrollable eye movement, vision difficulties (including decreased vision, double vision, or total loss of vision)
Hand tremor
Lack of control over the bladder or bowels
Loss of balance or coordination, clumsiness, trouble walking
Muscle weakness in the face, arm, or leg (usually on just one side)
Numbness or tingling on one side of the body
Personality, mood, behavior, or emotional changes
Trouble speaking or understanding others who are speaking
Other symptoms that may occur with a pituitary tumor:
Abnormal nipple discharge
Absent menstruation (periods)
Breast development in men
Enlarged hands, feet
Excessive body hair
Facial changes
Low blood pressure
Obesity
Sensitivity to heat or cold
Exams and Tests
The following tests may confirm the presence of a brain tumor and find its location:
CT scan of the head
EEG
Examination of tissue removed from the tumor during surgery or CT-guided biopsy (may confirm the type of tumor)
Examination of the cerebral spinal fluid (CSF) (may show cancerous cells)
MRI of the head
Treatment
Treatment can involve surgery, radiation therapy, and chemotherapy. Brain tumors are best treated by a team that includes:
Neuro-oncologist
Neurosurgeon
Medical oncologist
Radiation oncologist
Other health care providers, such as neurologists and social workers
Early treatment often improves the chance of a good outcome. Treatment depends on the size and type of tumor and your general health. Goals of treatment may be to cure the tumor, relieve symptoms, and improve brain function or comfort.
Surgery is often needed for most primary brain tumors. Some tumors may be completely removed. Those that are deep inside the brain or that enter brain tissue may be debulked instead of removed. Debulking is a procedure to reduce the tumor's size.
Tumors can be hard to remove completely by surgery alone. This is because the tumor invades surrounding brain tissue much like roots from a plant spread through soil. When the tumor cannot be removed, surgery may still help reduce pressure and relieve symptoms.
Radiation therapy is used for certain tumors.
Chemotherapy may be used with surgery or radiation treatment.
Other medicines used to treat primary brain tumors in children may include:
Medicines to reduce brain swelling and pressure
Anticonvulsants to reduce seizures
Pain medicines
Comfort measures, safety measures, physical therapy, and occupational therapy may be needed to improve quality of life. Counseling, support groups, and similar measures can help people cope with the disorder.
You may consider enrolling in a clinical trial after talking with your treatment team.
Legal advice may be helpful for creating advance directives such as a power of attorney.
Possible Complications
Brain herniation (often fatal)
Loss of ability to interact or function
Permanent, worsening, and severe loss of brain function
Return of tumor growth
Side effects of medications, including chemotherapy
Side effects of radiation treatments
When to Contact a Medical Professional
Call your health care provider if you develop any new, persistent headaches or other symptoms of a brain tumor.
Call your provider or go to the emergency room if you start having seizures, or suddenly develop stupor (reduced alertness), vision changes, or speech changes.
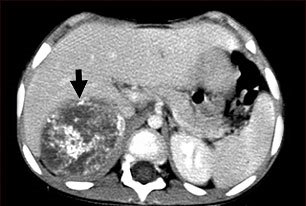
Neuroblastoma is a malignant (cancerous) tumor that develops from nerve tissue. It usually occurs in infants and children.
This CT scan of the upper abdomen shows a large tumor (neuroblastoma) on the person's right side (lower left side of picture). The tumor is behind the liver and is pushing the liver forward and may have possibly spread into the liver tissue.
Neuroblastoma can occur in many areas of the body. It develops from the tissues that form the sympathetic nervous system. This is the part of the nervous system that controls body functions, such as heart rate and blood pressure, digestion, and levels of certain hormones.
Most neuroblastomas begin in the abdomen in the adrenal gland or next to the spinal cord, or in the chest. Neuroblastomas can spread to the bones, such as in the face, skull, pelvis, shoulders, arms, and legs. It can also spread to bone marrow, liver, lymph nodes, skin, and around the eyes (orbits).
The cause of the tumor is unknown. Neuroblastoma is most commonly diagnosed in children before age 5. Each year there are around 700 new cases. The disorder occurs in approximately 1 out of 100,000 children and is slightly more common in boys.
In most patients, the neuroblastoma has already spread when it is first diagnosed.
In certain cases, surgery alone is enough. Often, though, other therapies are needed. Anticancer medications (chemotherapy) may be recommended if the tumor has spread. Radiation therapy may also be used.
High-dose chemotherapy, followed by autologous stem cell transplantation, is being studied for use in children with very high-risk tumors.
Support Groups
The stress of illness can be eased by joining a cancer support group. Sharing with others who have common experiences and problems and help you and your child not feel alone.
The outcome varies. In very young children with neuroblastoma, the tumor may go away on its own, without treatment. Or, the tissues of the tumor may mature and develop into a non-cancerous (benign) tumor called a ganglioneuroma, which can be surgically removed. In other cases, the tumor spreads quickly.
Response to treatment also varies. Treatment is often successful if the cancer has not spread. If it has spread, neuroblastoma is harder to cure. Younger children often do better than older children.
Tumors with certain genetic characteristics may be harder to cure.
Children treated for neuroblastoma may be at risk of getting a second, different cancer in the future.
Call your health care provider if your child has symptoms of neuroblastoma. Early diagnosis and treatment improves the chance of a good outcome.
Your salivary glands make saliva - sometimes called spit - and empty it into your mouth through openings called ducts. Saliva makes your food moist, which helps you chew and swallow. It helps you digest your food. It also cleans your mouth and contains antibodies that can kill germs.
Salivary gland cancer is a type of head and neck cancer. It is rare. It may not cause any symptoms, or you could notice
A lump in your ear, cheek, jaw, lip, or inside the mouth
Fluid draining from your ear
Trouble swallowing or opening the mouth widely
Numbness, weakness, or pain in your face
Doctors diagnose salivary gland cancer using a physical exam, imaging tests, and a biopsy. Treatment can include surgery, radiation therapy, and/or chemotherapy
Vulvar cancer is a rare type of cancer. It forms in a woman's external genitals, called the vulva. The cancer usually grows slowly over several years. First, precancerous cells grow on vulvar skin. This is called vulvar intraepithelial neoplasia (VIN), or dysplasia. Not all VIN cases turn into cancer, but it is best to treat it early.
Often, vulvar cancer doesn't cause symptoms at first. However, see your doctor for testing if you notice
A lump in the vulva
Vulvar itching or tenderness
Bleeding that is not your period
Changes in the vulvar skin, such as color changes or growths that look like a wart or ulcer
You are at greater risk if you've had a human papillomavirus (HPV) infection or have a history of genital warts. Your health care provider diagnoses vulvar cancer with a physica1 exam and a biopsy. Treatment varies, depending on your overall health and how advanced the cancer is. It might include surgery, radiation therapy, chemotherapy, or biologic therapy. Biologic therapy boosts your body's own ability to fight cancer.
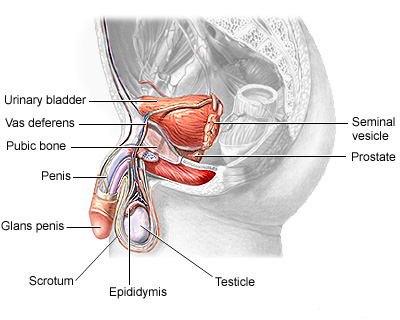
Smegma, a cheese-like, foul-smelling substance found under the foreskin of the penis may increase the risk of penis cancer.
Uncircumcised men who do not keep the area under the foreskin clean and men with a history of genital wartsor human papillomavirus (HPV) are at higher risk for this rare disorder.
The health care provider will perform a physical exam, which may reveal a non-tender lesion that looks like a pimple or wart. This growth is typically near the end of the penis.
A biopsy of the growth is needed to determine if it is cancer.
Treatment depends on the size and location of the tumor and how much it has spread.
In general, cancer treatment includes:
Chemotherapy -- uses medicines to kill cancer cells
Radiation -- using high powered x-rays to kill cancer cells
Surgery - cuts out and removes the cancer
If the tumor is small or near the tip of the penis, surgery may be done to remove only the cancerous part of the penis. Depending on the exact location, this is called a glansectomy or partial penectomy. Laser surgery may be used to treat some tumors.
For more severe tumors, total removal of the penis (total penectomy) is often necessary. A new opening will be created in the groin area to allow urine to exit the body. This procedure is called a urethrostomy.
Chemotherapy may be used along with surgery. Cisplatin, ifosfamide, and paclitaxel are usually used for treating penile cancer.
Radiation therapy is often recommended in combination with surgery. A type of radiation therapy called external beam therapy is often used. This method delivers radiation to the penis from outside the body. External beam radiation therapy is usually performed 5 days a week for 6 - 8 weeks.
The outcome can be good with early diagnosis and treatment. The 5-year survival rate for penile cancers is 65%. Urination and sexual function can often be maintained even when a significant portion of the penis is removed.
Circumcision may decrease the risk. Men who are not circumcised should be taught at an early age the importance of cleaning beneath the foreskin as part of their personal hygiene.
Good personal hygiene and safer sexual practices, such as abstinence, limiting the number of sexual partners, and use of condoms to prevent HPV infection, may decrease the risk of developing penile cancer.
 Матка имеет шейку, которая представляет собой сужение, расположенной в нижней части матки. Широкая часть матки, расположенная выше шейки, называется телом матки. Куполообразная верхняя часть органа называется дном матки. Фаллопиевы трубы представляют собой отростки матки, расположенные по обе стороны органа. Они заканчиваются яичниками.
Матка имеет шейку, которая представляет собой сужение, расположенной в нижней части матки. Широкая часть матки, расположенная выше шейки, называется телом матки. Куполообразная верхняя часть органа называется дном матки. Фаллопиевы трубы представляют собой отростки матки, расположенные по обе стороны органа. Они заканчиваются яичниками.