A lack of vitamin K causes hemorrhagic disease of the newborn. Vitamin K plays an important role in blood clotting.
Babies usually have low levels of vitamin K for a variety of reasons. Vitamin K doesn't move easily across the placenta from the mother to the baby. As a result, a newborn doesn't have much vitamin K stored up at birth. Also, there isn't much vitamin K in breast milk.
Your baby may develop this condition if:
A preventive vitamin K shot is not given at birth (if vitamin K is given by mouth instead of as a shot, it must be given more than once and it may not be as effective)
You take certain anti-seizure or blood thinning drugs
The condition is grouped into three categories:
Early onset hemorrhagic disease of the newborn is very rare. It occurs during the first hours of birth and certainly within 24 hours. Use of anti-seizure drugs or a blood thinner called coumadin during pregnancy is a common cause.
Classic onset disease may be seen in breastfed infants who did not receive a vitamin K shot within the first week after birth. It is also rare.
The late onset form is seen in infants older than 2 weeks up to 2 months old. It is more common in children who did not receive a vitamin K shot, and in those of Asian descent.
Newborns and infants with the following problems are more likely to develop this disorder:
The outlook tends to be worse for babies with late onset hemorrhagic disease than other forms. There is a higher rate of bleeding inside the skull (intracranial hemorrhage) associated with the late onset condition.
Vulvar cancer is a rare type of cancer. It forms in a woman's external genitals, called the vulva. The cancer usually grows slowly over several years. First, precancerous cells grow on vulvar skin. This is called vulvar intraepithelial neoplasia (VIN), or dysplasia. Not all VIN cases turn into cancer, but it is best to treat it early.
Often, vulvar cancer doesn't cause symptoms at first. However, see your doctor for testing if you notice
A lump in the vulva
Vulvar itching or tenderness
Bleeding that is not your period
Changes in the vulvar skin, such as color changes or growths that look like a wart or ulcer
You are at greater risk if you've had a human papillomavirus (HPV) infection or have a history of genital warts. Your health care provider diagnoses vulvar cancer with a physica1 exam and a biopsy. Treatment varies, depending on your overall health and how advanced the cancer is. It might include surgery, radiation therapy, chemotherapy, or biologic therapy. Biologic therapy boosts your body's own ability to fight cancer.
Uterine fibroids are common. As many as 1 in 5 women may have fibroids during their childbearing years. Half of all women have fibroids by age 50.
Fibroids are rare in women under age 20. They are more common in African-Americans than Caucasians.
No one knows exactly what causes fibroids. They are thought to be caused by:
Hormones in the body
Genes (may run in families)
Fibroids can be so tiny that you need a microscope to see them. They can also grow very large. They may fill the entire uterus and may weigh several pounds. Although it is possible for just one fibroid to develop, usually there are more than one.
Fibroids can grow:
In the muscle wall of the uterus (myometrial)
Just under the surface of the uterine lining (submucosal)
Just under the outside lining of the uterus (subserosal)
On a long stalk on the outside the uterus or inside the uterus (pedunculated)
Heavy bleeding during your period, sometimes with blood clots
Periods that may last longer than normal
Needing to urinate more often
Pelvic cramping or pain with periods
Feeling fullness or pressure in your lower belly
Pain during intercourse
Often, you can have fibroids and not have any symptoms. Your health care provider may find them during a physical exam or other test. Fibroids often shrink and cause no symptoms in women who have gone through menopause. A recent study also showed that some small fibroids shrink in premenopausal women.
Treatment for the symptoms of fibroids may include:
Birth control pills to help control heavy periods
Intrauterine devices (IUDs) that release hormones to help reduce heavy bleeding and pain
Iron supplements to prevent or treat anemia due to heavy periods
Pain relievers such as ibuprofen or naprosyn for cramps or pain
Hormone therapy shots to help shrink fibroids (done only for a short time)
Watchful waiting: You may have pelvic exams or ultrasounds every once in a while to check the fibroid's growth
Surgery and procedures used to treat fibroids include:
Hysteroscopy. This procedure can remove fibroids growing inside the uterus.
Uterine artery embolization.This procedure stops the blood supply to the fibroid, causing it to shrink and die. This may be a good option if you want to have children in the future.
Myomectomy. This surgery removes the fibroids from the uterus. This also may be a good choice if you want to have children. It won't prevent fibroids from growing again.
Hysterectomy. This surgery removes the uterus completely. It may be an option if you don't want children, medicines do not work, and you cannot have any other procedures.
If you have fibroids without symptoms, you may not need treatment.
If you have fibroids, they may grow if you become pregnant. This is due to the increased blood flow and higher estrogen levels. The fibroids usually return to their original size after your baby is born.
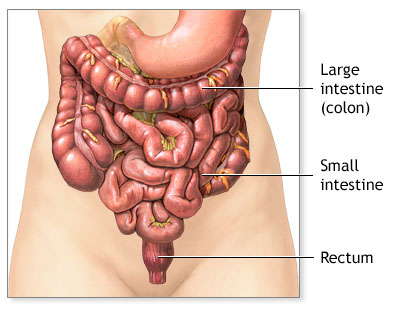
Ulcerative colitis is a type of inflammatory bowel disease (IBD) that affects the lining of the large intestine (colon) and rectum. Crohn's disease is a related condition.
Causes
The cause of ulcerative colitis is unknown. People with this condition have problems with the immune system, but it is not clear whether immune problems cause this illness. Although stress and certain foods can trigger symptoms, they do not cause ulcerative colitis.
Ulcerative colitis may affect any age group, although there are peaks at ages 15 - 30 and then again at ages 50 - 70.
The disease can begin the rectal area, and may involve the entire large intestine over time. It may also start in the rectum and other parts of the large intestine at the same time.
Risk factors include a family history of ulcerative colitis, or Jewish ancestry.
Symptoms
The symptoms vary in severity and may start slowly or suddenly. About half of people only have mild symptoms. Others have more severe attacks that occur more often. Many factors can lead to attacks, including respiratory infections or physical stress.
Colonoscopy with biopsy is generally used to diagnose ulcerative colitis.
Colonoscopy is also used to screen people with ulcerative colitis for colon cancer. Ulcerative colitis increases the risk of colon cancer. If you have this condition, you should be screened with colonoscopy about 8 - 12 years after being diagnosed. You should have a follow-up colonoscopy every 1 - 2 years.
Other tests that may be done to help diagnose this condition include:
Barium enema
Complete blood count (CBC)
C-reactive protein (CRP)
Sedimentation rate (ESR)
Treatment
The goals of treatment are to:
Control the acute attacks
Prevent repeated attacks
Help the colon heal
Hospitalization is often needed for severe attacks. Your doctor may prescribe corticosteroids to reduce inflammation. You may be given nutrients through a vein (intravenous line).
DIET AND NUTRITION
Certain types of foods may worsen diarrhea and gas symptoms, especially during times of active disease. Diet suggestions include:
Eat small amounts of food throughout the day.
Drink plenty of water (drink small amounts throughout the day).
Avoid high-fiber foods (bran, beans, nuts, seeds, and popcorn).
Avoid fatty, greasy or fried foods and sauces (butter, margarine, and heavy cream).
Limit milk products if you are lactose intolerant. Dairy products are a good source of protein and calcium.
STRESS
You may feel worried, embarrassed, or even sad or depresed about having a bowel accident. Other stressful events in your life, such as moving, or losing a job or a loved one can cause digestive problems.
Ask your doctor or nurse for tips on your to manage your stress.
MEDICATION
Medicines that may be used to decrease the number of attacks include:
5-aminosalicylates such as mesalamine or sulfazine, which can help control moderate symptoms
Immunomodulators such as azathioprine and 6-mercaptopurine
Corticosteroids (prednisone and methylprednisolone) taken by mouth during a flare-up or as a rectal suppository, foam, or enema
Infliximab (Remicade) or other biological treatments, if you do not respond to other medications
SURGERY
Surgery to remove the colon will cure ulcerative colitis and removes the threat of colon cancer. Surgery is usually recommended if you have:
Colitis that does not respond to complete medical therapy
Changes in the lining of the colon that are thought to be precancerous
Serious complications such as rupture (perforation) of the colon, severe bleeding (hemorrhage), or toxic megacolon
Most of the time, the entire colon, including the rectum, is removed (total proctocolectomy with ileostomy). Afterwards, you may need a surgical opening in the abdominal wall (ileostomy), or a procedure that connects the small intestine to the anus to gain more normal bowel function.
Outlook (Prognosis)
Symptoms are mild in about half of people with ulcerative colitis. You are less likely to respond well to medicines if your disease is more severe.
Permanent and complete control of symptoms with medications is unusual. Cure is only possible through complete removal of the large intestine.
The risk of colon cancer increases in each decade after ulcerative colitis is diagnosed.
Possible Complications
Repeated swelling (inflammation) leads to thickening of the intestinal wall and rectum with scar tissue. Death of colon tissue or severe infection (sepsis) may occur with severe disease.