A stroke is a medical emergency. Strokes happen when blood flow to your brain stops. Within minutes, brain cells begin to die. There are two kinds of stroke. The more common kind, called ischemic stroke, is caused by a blood clot that blocks or plugs a blood vessel in the brain. The other kind, called hemorrhagic stroke, is caused by a blood vessel that breaks and bleeds into the brain. "Mini-strokes" or transient ischemic attacks (TIAs), occur when the blood supply to the brain is briefly interrupted.
Symptoms of stroke are:
Sudden numbness or weakness of the face, arm or leg (especially on one side of the body)
Sudden confusion, trouble speaking or understanding speech
Sudden trouble seeing in one or both eyes
Sudden trouble walking, dizziness, loss of balance or coordination
Sudden severe headache with no known cause
If you have any of these symptoms, you must get to a hospital quickly to begin treatment. Acute stroke therapies try to stop a stroke while it is happening by quickly dissolving the blood clot or by stopping the bleeding. Post-stroke rehabilitation helps individuals overcome disabilities that result from stroke damage. Drug therapy with blood thinners is the most common treatment for stroke.
Types of Stroke
ISCHEMIC STROKE
An ischemic stroke occurs if an artery that supplies oxygen-rich blood to the brain becomes blocked. Blood clots often cause the blockages that lead to ischemic strokes.
The two types of ischemic stroke are thrombotic and embolic. In a thrombotic stroke, a blood clot (thrombus) forms in an artery that supplies blood to the brain.
In an embolic stroke, a blood clot or other substance (such as plaque, a fatty material) travels through the bloodstream to an artery in the brain. (A blood clot or piece of plaque that travels through the bloodstream is called an embolus.)
With both types of ischemic stroke, the blood clot or plaque blocks the flow of oxygen-rich blood to a portion of the brain.
HEMORRHAGIC STROKE
A hemorrhagic stroke occurs if an artery in the brain leaks blood or ruptures (breaks open). The pressure from the leaked blood damages brain cells.
The two types of hemorrhagic stroke are intracerebral and subarachnoid. In an intracerebral hemorrhage, a blood vessel inside the brain leaks blood or ruptures.
In a subarachnoid hemorrhage, a blood vessel on the surface of the brain leaks blood or ruptures. When this happens, bleeding occurs between the inner and middle layers of the membranes that cover the brain.
In both types of hemorrhagic stroke, the leaked blood causes swelling of the brain and increased pressure in the skull. The swelling and pressure damage cells and tissues in the brain.
What Causes a Stroke?
ISCHEMIC STROKE AND TRANSIENT ISCHEMIC ATTACK
An ischemic stroke or transient ischemic attack (TIA) occurs if an artery that supplies oxygen-rich blood to the brain becomes blocked. Many medical conditions can increase the risk of ischemic stroke or TIA.
For example, atherosclerosis is a disease in which a fatty substance called plaque builds up on the inner walls of the arteries. Plaque hardens and narrows the arteries, which limits the flow of blood to tissues and organs (such as the heart and brain).
Plaque in an artery can crack or rupture (break open). Blood platelets, which are disc-shaped cell fragments, stick to the site of the plaque injury and clump together to form blood clots. These clots can partly or fully block an artery.
Plaque can build up in any artery in the body, including arteries in the heart, brain, and neck. The two main arteries on each side of the neck are called the carotid arteries. These arteries supply oxygen-rich blood to the brain, face, scalp, and neck.
When plaque builds up in the carotid arteries, the condition is called carotid artery disease. Carotid artery disease causes many of the ischemic strokes and TIAs that occur in the United States.
An embolic stroke (a type of ischemic stroke) or TIA also can occur if a blood clot or piece of plaque breaks away from the wall of an artery. The clot or plaque can travel through the bloodstream and get stuck in one of the brain’s arteries. This stops blood flow through the artery and damages brain cells.
Heart conditions and blood disorders also can cause blood clots that can lead to a stroke or TIA. For example, atrial fibrillation, or AF, is a common cause of embolic stroke.
In AF, the upper chambers of the heart contract in a very fast and irregular way. As a result, some blood pools in the heart. The pooling increases the risk of blood clots forming in the heart chambers.
An ischemic stroke or TIA also can occur because of lesions caused by atherosclerosis. These lesions may form in the small arteries of the brain, and they can block blood flow to the brain.
HEMORRHAGIC STROKE
Sudden bleeding in the brain can cause a hemorrhagic stroke. The bleeding causes swelling of the brain and increased pressure in the skull. The swelling and pressure damage brain cells and tissues.
Examples of conditions that can cause a hemorrhagic stroke include high blood pressure, aneurysms, and arteriovenous malformations (AVMs).
"Blood pressure" is the force of blood pushing against the walls of the arteries as the heart pumps blood. If blood pressure rises and stays high over time, it can damage the body in many ways.
Aneurysms are balloon-like bulges in an artery that can stretch and burst. AVMs are tangles of faulty arteries and veins that can rupture within the brain. High blood pressure can increase the risk of hemorrhagic stroke in people who have aneurysms or AVMs.
Who Is at Risk for a Stroke?
Certain traits, conditions, and habits can raise your risk of having a stroke or transient ischemic attack (TIA). These traits, conditions, and habits are known as risk factors.
The more risk factors you have, the more likely you are to have a stroke. You can treat or control some risk factors, such as high blood pressure and smoking. Other risk factors, such as age and gender, you can’t control.
The major risk factors for stroke include:
High blood pressure. High blood pressure is the main risk factor for stroke. Blood pressure is considered high if it stays at or above 140/90 mmHg over time. If you have diabetes or chronic kidney disease, high blood pressure is defined as 130/80 mmHg or higher. (The mmHg is millimeters of mercury—the units used to measure blood pressure.)
Smoking. Smoking can damage blood vessels and raise blood pressure. Smoking also may reduce the amount of oxygen that reaches your body's tissues. Exposure to secondhand smoke also can damage the blood vessels.
Diabetes. Diabetes is a disease in which the blood sugar level is high because the body doesn't make enough insulin or doesn't use its insulin properly. Insulin is a hormone that helps move blood sugar into cells where it’s used for energy.
Heart diseases. Coronary heart disease (also called coronary artery disease), cardiomyopathy, heart failure, and atrial fibrillation can cause blood clots that can lead to a stroke.
Brain aneurysms or arteriovenous malformations (AVMs). Aneurysms are balloon-like bulges in an artery that can stretch and burst. AVMs are tangles of faulty arteries and veins that can rupture (break open) within the brain. AVMs may be present at birth, but often aren’t diagnosed until they rupture.
Age and gender. Your risk of stroke increases as you get older. At younger ages, men are more likely than women to have strokes. However, women are more likely to die from strokes. Women who take birth control pills also are at slightly higher risk of stroke.
Race and ethnicity. Strokes occur more often in African American, Alaska Native, and American Indian adults than in Caucasian, Hispanic, or Asian American adults.
Personal or family history of stroke or TIA. If you’ve had a stroke, you’re at higher risk for another one. Your risk of having a repeat stroke is the highest right after a stroke. A TIA also increases your risk of having a stroke, as does having a family history of stroke.
Other risk factors for stroke, many of which of you can control, include:
Alcohol and illegal drug use, including cocaine, amphetamines, and other drugs
Certain medical conditions, such as vasculitis, inflammation of the blood vessels), and bleeding disorders
Following a healthy lifestyle can lower the risk of stroke. Some people also may need to take medicines to lower their risk.
Sometimes strokes can occur in people who don’t have any known risk factors.
What Are the Signs and Symptoms of a Stroke?
The signs and symptoms of a stroke often develop quickly. However, they can develop over hours or even days.
The type of symptoms depends on the type of stroke and the area of the brain that’s affected. How long symptoms last and how severe they are vary among different people.
Signs and symptoms of a stroke may include:
Sudden weakness
Paralysis (an inability to move) or numbness of the face, arms, or legs, especially on one side of the body
Confusion
Trouble speaking or understanding speech
Trouble seeing in one or both eyes
Problems breathing
Dizziness, trouble walking, loss of balance or coordination, and unexplained falls
A transient ischemic attack (TIA) has the same signs and symptoms as a stroke. However, TIA symptoms usually last less than 1–2 hours (although they may last up to 24 hours). A TIA may occur only once in a person’s lifetime or more often.
At first, it may not be possible to tell whether someone is having a TIA or stroke. All stroke-like symptoms require medical care.
If you think you or someone else is having a TIA or stroke, call 9–1–1 right away. Do not drive to the hospital or let someone else drive you. Call an ambulance so that medical personnel can begin life-saving treatment on the way to the emergency room. During a stroke, every minute counts.
Stroke Complications
After you’ve had a stroke, you may develop other complications, such as:
Blood clots and muscle weakness. Being immobile (unable to move around) for a long time can raise your risk of developing blood clots in the deep veins of the legs. Being immobile also can lead to muscle weakness and decreased muscle flexibility.
Problems swallowing and pneumonia. If a stroke affects the muscles used for swallowing, you may have a hard time eating or drinking. You also may be at risk of inhaling food or drink into your lungs. If this happens, you may develop pneumonia.
Loss of bladder control. Some strokes affect the muscles used to urinate. You may need a urinary catheter (a tube placed into the bladder) until you can urinate on your own. Use of these catheters can lead to urinary tract infections. Loss of bowel control or constipation also may occur after a stroke.
How Is a Stroke Diagnosed?
Your doctor will diagnose a stroke based on your signs and symptoms, your medical history, a physical exam, and test results.
Your doctor will want to find out the type of stroke you’ve had, its cause, the part of the brain that's affected, and whether you have bleeding in the brain.
If your doctor thinks you’ve had a transient ischemic attack (TIA), he or she will look for its cause to help prevent a future stroke.
Medical History and Physical Exam
Your doctor will ask you or a family member about your risk factors for stroke. Examples of risk factors include high blood pressure, smoking, heart disease, and a personal or family history of stroke. Your doctor also will ask about your signs and symptoms and when they began.
During the physical exam, your doctor will check your mental alertness and your coordination and balance. He or she will check for numbness or weakness in your face, arms, and legs; confusion; and trouble speaking and seeing clearly.
Your doctor will look for signs of carotid artery disease, a common cause of ischemic stroke. He or she will listen to your carotid arteries with a stethoscope. A whooshing sound called a bruit may suggest changed or reduced blood flow due to plaque buildup in the carotid arteries.
Diagnostic Tests and Procedures
Your doctor may recommend one or more of the following tests to diagnose a stroke or TIA.
Brain Computed Tomography
A brain computed tomography scan, or brain CT scan, is a painless test that uses x rays to take clear, detailed pictures of your brain. This test often is done right after a stroke is suspected.
A brain CT scan can show bleeding in the brain or damage to the brain cells from a stroke. The test also can show other brain conditions that may be causing your symptoms.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) uses magnets and radio waves to create pictures of the organs and structures in your body. This test can detect changes in brain tissue and damage to brain cells from a stroke.
An MRI may be used instead of, or in addition to, a CT scan to diagnose a stroke.
Computed Tomography Arteriogram and Magnetic Resonance Arteriogram
A CT arteriogram (CTA) and magnetic resonance arteriogram (MRA) can show the large blood vessels in the brain. These tests may give your doctor more information about the site of a blood clot and the flow of blood through your brain.
Carotid Ultrasound
Carotid ultrasound is a painless and harmless test that uses sound waves to create pictures of the insides of your carotid arteries. These arteries supply oxygen-rich blood to your brain.
Carotid ultrasound shows whether plaque has narrowed or blocked your carotid arteries.
Your carotid ultrasound test may include a Doppler ultrasound. Doppler ultrasound is a special test that shows the speed and direction of blood moving through your blood vessels.
Carotid Angiography
Carotid angiography is a test that uses dye and special x rays to show the insides of your carotid arteries.
For this test, a small tube called a catheter is put into an artery, usually in the groin (upper thigh). The tube is then moved up into one of your carotid arteries.
Your doctor will inject a substance (called contrast dye) into the carotid artery. The dye helps make the artery visible on x-ray pictures.
Heart Tests
EKG (Electrocardiogram)
An EKG is a simple, painless test that records the heart's electrical activity. The test shows how fast the heart is beating and its rhythm (steady or irregular). An EKG also records the strength and timing of electrical signals as they pass through each part of the heart. An EKG can help detect heart problems that may have led to a stroke. For example, the test can help diagnose atrial fibrillation or a previous heart attack.
Echocardiography
Echocardiography (EK-o-kar-de-OG-ra-fee), or echo, is a painless test that uses sound waves to create pictures of your heart.
The test gives information about the size and shape of your heart and how well your heart's chambers and valves are working.
Echo can detect possible blood clots inside the heart and problems with the aorta. The aorta is the main artery that carries oxygen-rich blood from your heart to all parts of your body.
Blood Tests
Your doctor also may use blood tests to help diagnose a stroke.
A blood glucose test measures the amount of glucose (sugar) in your blood. Low blood glucose levels may cause symptoms similar to those of a stroke.
A platelet count measures the number of platelets in your blood. Blood platelets are cell fragments that help your blood clot. Abnormal platelet levels may be a sign of a bleeding disorder (not enough clotting) or a thrombotic disorder (too much clotting).
Your doctor also may recommend blood tests to measure how long it takes for your blood to clot. Two tests that may be used are called PT and PTT tests. These tests show whether your blood is clotting normally.
How Is a Stroke Treated?
Treatment for a stroke depends on whether it is ischemic or hemorrhagic. Treatment for a transient ischemic attack (TIA) depends on its cause, how much time has passed since symptoms began, and whether you have other medical conditions.
Strokes and TIAs are medical emergencies. If you have stroke symptoms, call emergency right away. Do not drive to the hospital or let someone else drive you. Call an ambulance so that medical personnel can begin life-saving treatment on the way to the emergency room. During a stroke, every minute counts.
Once you receive initial treatment, your doctor will try to treat your stroke risk factors and prevent complications.
Treating Ischemic Stroke and Transient Ischemic Attack
An ischemic stroke or TIA occurs if an artery that supplies oxygen-rich blood to the brain becomes blocked. Often, blood clots cause the blockages that lead to ischemic strokes and TIAs.
Treatment for an ischemic stroke or TIA may include medicines and medical procedures.
Medicines
A medicine called tissue plasminogen activator (tPA) can break up blood clots in the arteries of the brain. A doctor will inject tPA into a vein in your arm. This medicine must be given within 4 hours of the start of symptoms to work. Ideally, it should be given as soon as possible.
If, for medical reasons, your doctor can’t give you tPA, you may get an antiplatelet medicine. For example, aspirin may be given within 48 hours of a stroke. Antiplatelet medicines help stop platelets from clumping together to form blood clots.
Your doctor also may prescribe anticoagulants, or “blood thinners.” These medicines can keep blood clots from getting larger and prevent new blood clots from forming.
Medical Procedures
If you have carotid artery disease, your doctor may recommend a carotid endarterectomy or carotid artery percutaneous coronary intervention, sometimes referred to as angioplasty. Both procedures open blocked carotid arteries.
Researchers are testing other treatments for ischemic stroke, such as intra-arterial thrombolysis and mechanical clot (embolus) removal in cerebral ischemia (MERCI).
In intra-arterial thrombolysis, a long flexible tube called a catheter is put into your groin (upper thigh) and threaded to the tiny arteries of the brain. Your doctor can deliver medicine through this catheter to break up a blood clot in the brain.
MERCI is a device that can remove blood clots from an artery. During the procedure, a catheter is threaded through a carotid artery to the affected artery in the brain. The device is then used to pull the blood clot out through the catheter.
Treating Hemorrhagic Stroke
A hemorrhagic stroke occurs if an artery in the brain leaks blood or ruptures (breaks open). The first steps in treating a hemorrhagic stroke are to find the cause of bleeding in the brain and then control it.
Unlike ischemic strokes, hemorrhagic strokes aren’t treated with antiplatelet medicines and blood thinners. This is because these medicines can make bleeding worse.
If you’re taking antiplatelet medicines or blood thinners and have a hemorrhagic stroke, you’ll be taken off the medicine.
If high blood pressure is the cause of bleeding in the brain, your doctor may prescribe medicines to lower your blood pressure. This can help prevent further bleeding.
Surgery also may be needed to treat a hemorrhagic stroke. The types of surgery used include aneurysm clipping, coil embolization (EM-bol-ih-ZA-shun), and arteriovenous malformation (AVM) repair.
Aneurysm Clipping and Coil Embolization
If an aneurysm (a balloon-like bulge in an artery) is the cause of a stroke, your doctor may recommend aneurysm clipping or coil embolization.
Aneurysm clipping is done to block off the aneurysm from the blood vessels in the brain. This surgery helps prevent further leaking of blood from the aneurysm. It also can help prevent the aneurysm from bursting again.
During the procedure, a surgeon will make an incision (cut) in the brain and place a tiny clamp at the base of the aneurysm. You’ll be given medicine to make you sleep during the surgery. After the surgery, you’ll need to stay in the hospital’s intensive care unit for a few days.
Coil embolization is a less complex procedure for treating an aneurysm. The surgeon will insert a tube called a catheter into an artery in the groin. He or she will thread the tube to the site of the aneurysm.
Then, a tiny coil will be pushed through the tube and into the aneurysm. The coil will cause a blood clot to form, which will block blood flow through the aneurysm and prevent it from bursting again.
Coil embolization is done in a hospital. You’ll be given medicine to make you sleep during the surgery.
Arteriovenous Malformation Repair
If an AVM is the cause of a stroke, your doctor may recommend an AVM repair. (An AVM is a tangle of faulty arteries and veins that can rupture within the brain.) AVM repair helps prevent further bleeding in the brain.
Doctors use several methods to repair AVMs. These methods include:
Surgery to remove the AVM
Injecting a substance into the blood vessels of the AVM to block blood flow
Using radiation to shrink the blood vessels of the AVM
Treating Stroke Risk Factors
After initial treatment for a stroke or TIA, your doctor will treat your risk factors. He or she may recommend lifestyle changes to help control your risk factors.
Lifestyle changes may include quitting smoking, following a healthy diet, maintaining a healthy weight, and being physically active.
If lifestyle changes aren’t enough, you may need medicine to control your risk factors.
Quitting Smoking
If you smoke or use tobacco, quit. Smoking can damage your blood vessels and raise your risk of stroke and other health problems. Talk with your doctor about programs and products that can help you quit. Also, try to avoid secondhand smoke. Secondhand smoke also can damage the blood vessels.
Following a Healthy Diet
A healthy diet is an important part of a healthy lifestyle. Choose a variety of fruits, vegetables, and grains; half of your grains should come from whole-grain products.
Choose foods that are low in saturated fat, trans fat, and cholesterol. Healthy choices include lean meats, poultry without skin, fish, beans, and fat-free or low-fat milk and milk products.
Choose and prepare foods with little sodium (salt). Too much salt can raise your risk of high blood pressure.
Choose foods and beverages that are low in added sugar. If you drink alcoholic beverages, do so in moderation.
Maintaining a Healthy Weight
Maintaining a healthy weight can lower your risk of stroke. A general goal to aim for is a body mass index (BMI) of less than 25.
BMI measures your weight in relation to your height and gives an estimate of your total body fat. You can measure your BMI using zdrav.kz resources – BMI, food pyramid, etc., or your health care provider can measure your BMI.
A BMI between 25 and 29.9 is considered overweight. A BMI of 30 or more is considered obese. A BMI of less than 25 is the goal for preventing a stroke.
Being Physically Active
Regular physical activity can help control many stroke risk factors, such as high blood pressure, unhealthy cholesterol levels, and excess weight.
Talk with your doctor before you start a new exercise plan. Ask him or her how much and what kinds of physical activity are safe for you.
People gain health benefits from as little as 60 minutes of moderate-intensity aerobic activity per week. The more active you are, the more you will benefit.
How Can a Stroke Be Prevented?
Taking action to control your risk factors can help prevent or delay a stroke. If you’ve already had a stroke, these actions can help prevent another one.
Don’t smoke. If you smoke or use tobacco, quit. Smoking can damage and tighten blood vessels and raise your risk of stroke. Talk with your doctor about programs and products that can help you quit. Also, try to avoid secondhand smoke. Secondhand smoke also can damage the blood vessels.
Make healthy eating choices. A healthy diet includes a variety of fruits, vegetables, and whole grains. It also includes lean meats, poultry, fish, beans, and fat-free or low-fat milk or milk products. A healthy diet is low in saturated fat, trans fat, cholesterol, sodium (salt), and added sugars.
Maintain a healthy weight. If you're overweight or obese, work with your doctor to create a reasonable weight-loss plan. Controlling your weight helps you control stroke risk factors.
Be as physically active as you can. Physical activity can improve your fitness level and your health. Talk with your doctor about what types and amounts of activity are safe for you.
Know your family history of stroke. If you or someone in your family has had a stroke, be sure to tell your doctor.
For more information about healthy lifestyle changes, go to previous section “How Is a Stroke Treated?” If lifestyle changes are not enough, you also may need medicines to control your stroke risk factors. Take all of your medicines as your doctor prescribes.
If you’ve had a transient ischemic attack (TIA), don’t ignore it. It’s important for your doctor to find the cause of the TIA so you can take steps to prevent a stroke.
Life After a Stroke
The time it takes to recover from a stroke varies—it can take weeks, months, or even years. Some people recover fully, while others have long-term or lifelong disabilities.
Ongoing care, rehabilitation, and emotional support can help you recover and may even help prevent another stroke.
If you’ve had a stroke, you’re at risk of having another one. Know the warning signs of a stroke and transient ischemic attack (TIA) and what to do if they occur. Call emergency as soon as symptoms start.
Do not drive to the hospital or let someone else drive you. Call an ambulance so that medical personnel can begin life-saving treatment on the way to the emergency room. During a stroke, every minute counts.
Ongoing Care
Lifestyle changes can help you recover from a stroke and may help prevent another one. Examples of these changes include quitting smoking, following a healthy diet, maintaining a healthy weight, and being physically active. Talk with your doctor about the types and amounts of physical activity that are safe for you.
Your doctor also may prescribe medicines to help you recover from a stroke or control your stroke risk factors. Take all of your medicines as your doctor prescribes.
If you had an ischemic stroke, you may need to take anticoagulants, also called blood thinners. These medicines prevent blood clots from getting larger and keep new clots from forming. You’ll likely need routine blood tests to check how well these medicines are working.
The most common side effect of blood thinners is bleeding. This happens if the medicine thins your blood too much. This side effect can be life threatening. Bleeding can occur inside your body cavities (internal bleeding) or from the surface of your skin (external bleeding).
Know the warning signs of bleeding so you can get help right away. They include:
Unexplained bruising and/or tiny red or purple dots on the skin
Unexplained bleeding from the gums and nose
Increased menstrual flow
Bright red vomit or vomit that looks like coffee grounds
Blood in your urine, bright red blood in your stools, or black tarry stools
A lot of bleeding after a fall or injury or easy bruising or bleeding also may mean that your blood is too thin. Call your doctor right away if you have any of these signs. If you have severe bleeding, call emergency.
Talk with your doctor about how often you should schedule followup visits or tests. These visits and tests can help your doctor monitor your stroke risk factors and adjust your treatment as needed.
Rehabilitation
After a stroke, you may need rehabilitation (rehab) to help you recover. Rehab may include working with speech, physical, and occupational therapists.
Language, Speech, and Memory
You may have trouble communicating after a stroke. You may not be able to find the right words, put complete sentences together, or put words together in a way that makes sense. You also may have problems with your memory and thinking clearly. These problems can be very frustrating.
Speech and language therapists can help you learn ways to communicate again and improve your memory.
Muscle and Nerve Problems
A stroke may affect only one side of the body or part of one side. It can cause paralysis (an inability to move) or muscle weakness, which can put you at risk for falling.
Physical and occupational therapists can help you strengthen and stretch your muscles. They also can help you relearn how to do daily activities, such as dressing, eating, and bathing.
Bladder and Bowel Problems
A stroke can affect the muscles and nerves that control the bladder and bowels. You may feel like you have to urinate often, even if your bladder isn’t full. You may not be able to get to the bathroom in time. Medicines and a bladder or bowel specialist can help with these problems.
Swallowing and Eating Problems
You may have trouble swallowing after a stroke. Signs of this problem are coughing or choking during eating or coughing up food after eating.
A speech therapist can help you with these issues. He or she may suggest changes to your diet, such as eating puréed (finely chopped) foods or drinking thick liquids.
Emotional Issues and Support
After a stroke, you may have changes in your behavior or judgment. For example, your mood may change quickly. Because of these and other changes, you may feel scared, anxious, and depressed. Recovering from a stroke can be slow and frustrating.
Talk about how you feel with your health care team. Talking to a professional counselor also can help. If you’re very depressed, your doctor may recommend medicines or other treatments that can improve your quality of life.
Priapism is a prolonged erection of the penis. The unwanted, persistent erection isn't caused by sexual stimulation or arousal, and priapism is usually painful.
Priapism is an uncommon condition that needs immediate medical attention. Prompt treatment for priapism is usually needed to prevent tissue damage that could result in the inability to get or maintain an erection (erectile dysfunction).
Priapism is most common between ages 5 and 10 in boys and ages 20 and 50 in men.
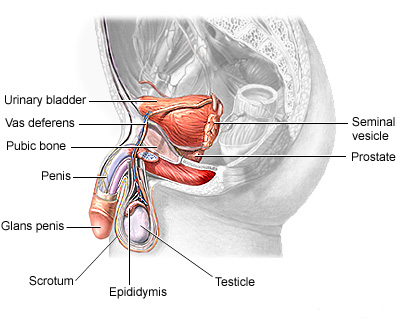
Male reproductive system
Priapism causes abnormally persistent erections not related to sexual stimulation. Priapism symptoms may vary depending on the type of priapism. There are two main types: ischemic and nonischemic priapism.
Ischemic priapism
Ischemic, also called low-flow, priapism is the result of blood not being able to leave the penis. It's the more common type of priapism. Signs and symptoms include:
Unwanted erection lasting more than four hours
Unwanted erection off and on for several hours (stuttering priapism)
Rigid penile shaft, but usually soft tip of penis (glans)
Usually painful or tender penis
Nonischemic priapism
Nonischemic, or high-flow, priapism occurs when too much blood flows into the penis. Nonischemic priapism is usually painless. Signs and symptoms include:
Unwanted erection lasting at least four hours
Erect but not rigid penile shaft
When to see a doctor
If you have an erection lasting longer than four hours, go to the emergency room. If you experience a painful, persistent erection that resolves on its own in less than four hours, see your doctor. You may need treatment to prevent further episodes.
An erection normally occurs in response to physical or psychological stimulation. This stimulation causes certain blood vessels to relax and expand, increasing blood flow to spongy tissues in the penis. Consequently, the blood-filled penis becomes erect. After stimulation ends, the blood flows out, and the penis returns to its nonrigid (flaccid) state.
Priapism occurs when some part of this system — the blood, blood vessels or nerves — changes normal blood flow. Subsequently, an unwanted erection persists. Factors that can contribute to priapism include the following.
Blood disorders, such as Leukemia
Prescription medications, such as antidepressants, blood thinners
Alcohol and drug use
Injury
Other factors, such as Blood clots, Spinal cord injury
In some cases, doctors are unable to identify the specific cause for priapism.
Ischemic priapism can cause serious complications. The blood trapped in the penis is deprived of oxygen. When an erection lasts for longer than four hours, this oxygen-poor blood can begin to damage or destroy tissues in the penis. As a result, untreated priapism may cause:
Erectile dysfunction, the inability of the penis to become or stay erect with sexual arousal
Disfigurement of the penis
If you or your child has experienced a painful, persistent erection that lasted less than four hours, or multiple unwanted, persistent erections (stuttering priapism), see your primary care doctor. If the erection has lasted more than four hours, go to the emergency room.
Your doctor or the emergency room doctor may suggest that you make a follow-up appointment with a specialist in reproductive and urinary organs (urologist).
If you have time before you see your doctor, it's a good idea to prepare for questions the doctor is likely to ask.
What you can do
Write down the symptoms, including any that may seem unrelated to the persistent erections.
Make a list of all medications, as well as any vitamins or supplements, that you're taking. And, let your doctor know if you've taken any nutritional supplements or illegal drugs.
You may also want to prepare a list of questions to ask the doctor:
What is likely causing the persistent erections?
What kind of tests might be needed?
What can be done to prevent this problem in the future?
If medication is necessary, is there a generic alternative?
Are there activities, such as exercise or sex, that should be avoided? If so, for how long?
Does priapism increase the risk of developing erectile dysfunction?
Do you have brochures or can you suggest websites that explain more about priapism?
If other questions occur to you or you don't understand something, don't hesitate to ask questions during your appointment.
What to expect from your doctor
Your doctor is likely to ask a number of questions regarding recurring episodes of persistent erections. Your doctor may ask:
When did your symptoms first start?
How long have the erections lasted?
Were the erections painful?
Have you had an injury to your genitals or groin?
Did the unwanted erections occur after using a particular substance, such as alcohol, marijuana, cocaine or other drugs?
Do you take any prescription medications, including drugs for treating erectile dysfunction? Do you take any herbal or dietary supplements?
Your doctor may also order laboratory tests to determine if a disease or condition is causing priapism.
What you can do in the meantime
Don't stop your prescription medications without consulting your doctor. Don't use any recreational substance that could cause persistent erections.
If you have an erection lasting more than four hours, you need emergency care. The emergency room doctor will determine first whether you have ischemic priapism or nonischemic priapism. This is necessary because the treatment for each is different, and treatment for ischemic priapism needs to be done as soon as possible.
Medical history and exam
To determine what type of priapism you have, your doctor will likely ask numerous questions and examine your genitals, abdomen, groin and perineum. He or she may be able to determine what type of priapism you have based on the rigidity and sensitivity of the penis. This exam may also reveal signs of injury or tumors that could be causing priapism. An injury, for example, would suggest that nonischemic priapism is more likely.
Diagnostic tests
Diagnostic tests may be necessary to determine what type of priapism you have. Additional tests may identify the cause of priapism. In an emergency room setting, your treatment may begin before all test results are received if the doctor is confident about what kind of priapism you have. Diagnostic tests include:
Blood gas measurement. In this test, a tiny needle is inserted into your penis to remove a sample of blood. If the blood is dark — deprived of oxygen — the condition is most likely ischemic priapism. If it's bright red, the priapism is most likely nonischemic. A laboratory test measuring the amounts of certain gases in the blood can confirm the type of priapism.
Blood tests. Your blood can be tested to measure the number of red blood cells and platelets present. Results may provide evidence of diseases, such as sickle cell anemia, other blood disorders or certain cancers.
Ultrasound. You may have color duplex ultrasonography, which uses sound waves to create an image of internal organs. This test can be used to measure blood flow within your penis that would suggest ischemic or nonischemic priapism. The exam may also reveal an injury, tumor or abnormality that may be an underlying cause.
Toxicology test. Your doctor may order a test to screen for illegal or prescription drugs that may be the cause of priapism. This test may be done with blood or urine samples.
Ischemic priapism
Ischemic priapism — the result of blood not being able to exit the penis — is an emergency situation that requires immediate treatment. This treatment usually begins with a combination of draining blood from the penis and using medications.
Aspiration. After your penis is numbed with local anesthetic, excess blood is drained from it, using a small needle and syringe. As part of this procedure, the penile veins may also be flushed with a saline solution. This treatment relieves pain, removes oxygen-poor blood and may stop the erection. This treatment may be repeated until the erection ends.
Medication. A medication called an alpha-adrenergic sympathomimetic, such as phenylephrine, may be injected into the spongy tissue of the penis. This drug constricts blood vessels that carry blood into the penis. This action allows blood vessels that carry blood out of the penis to open up and allow increased blood flow out. This treatment may be repeated over several hours if necessary. There is some risk of side effects, such as headache, dizziness and high blood pressure, particularly if you have high blood pressure or heart disease.
Surgery. If other treatments aren't successful, a surgeon may implant a device that reroutes blood flow (a shunt) so that blood can move through your penis normally.
Additional treatments. If you have sickle cell anemia, you may receive additional treatments that are used to treat disease-related episodes, such as supplemental oxygen or an intravenous solution to keep you hydrated.
Nonischemic priapism
Nonischemic priapism often goes away with no treatment. Because there isn't a risk of damage to the penis, your doctor may suggest a watch-and-wait approach. Putting ice and pressure on the perineum — the region between the base of the penis and the anus — may help end the erection.
Surgery may be necessary in some cases to insert material that temporarily blocks blood flow to the penis. The body eventually absorbs the material. Surgery may also be necessary to repair arteries or tissue damage resulting from an injury.
Depending on the probable cause of the priapism, steps to prevent recurrent priapism may include:
Treating the disease that may have caused priapism
Changing medications if a prescription medication was the probable cause
Avoiding triggers, such as alcohol or illegal drugs
Self-injection of phenylephrine to stop prolonged erections