You haven't been feeling so great for the last few days, and you've had a runny nose and a cough. Then one morning you wake up and stumble into the bathroom. You look in the mirror with blurry eyes and — yikes! You have chickenpox!
What Is Chickenpox?
Chickenpox is caused by a virus called varicella zoster. People who get the virus often develop a rash of spots that look like blisters all over their bodies. The blisters are small and sit on an area of red skin that can be anywhere from the size of a pencil eraser to the size of a dime.
You've probably heard that chickenpox are itchy. It's true. The illness also may come along with a runny nose and cough. But the good news is that chickenpox is a common illness for kids, and most get better by resting just like you do with a cold or the flu.
And the really good news is that, thanks to the chickenpox vaccine, lots of kids don't get chickenpox at all. Kids who do get it after they've gotten the shot often get less severe cases, which means they get better quicker.
What Happens When You Have Chickenpox?
Chickenpox may start out seeming like a cold: You might have a runny or stuffy nose, sneezing, and a cough. But 1 to 2 days later, the rash begins, often in bunches of spots on the chest and face. From there it can spread out quickly over the entire body — sometimes the rash is even in a person's ears and mouth.
The number of pox is different for everyone. Some people get just a few bumps; others are covered from head to toe. At first, the rash looks like pinkish dots that quickly develop a small blister on top (a blister is a bump on your skin that fills up with fluid). After about 24 to 48 hours, the fluid in the blisters gets cloudy and the blisters begin to crust over.
Chickenpox blisters show up in waves, so after some begin to crust over, a new group of spots might appear. New chickenpox usually stop appearing by the seventh day, though they may stop as early as the third day. It usually takes 10–14 days for all the blisters to be scabbed over and then you are no longer contagious.
Besides the rash, someone with chickenpox might also have a stomachache, a fever, and may just not feel well.
How Does Chickenpox Spread?
Chickenpox is contagious, meaning that someone who has it can easily spread it to someone else. Someone who has chickenpox is most contagious during the first 2 to 5 days of being sick. That's usually about 1 to 2 days before the rash shows up. So you could be spreading around chickenpox without even knowing it!
A person who has chickenpox can pass it to someone else by coughing or sneezing. When he or she coughs, sneezes, laughs, and even talks, tiny drops come out of the mouth and nose. These drops are full of the chickenpox virus. It's easy for others to breathe in these drops or get them on their hands. Before you know it, the chickenpox virus has infected someone new.
Itchy-Itchy, Scratchy-Scratchy
If you are that unlucky person, how do you keep your chickenpox from driving you crazy? They itch, but you're not supposed to scratch them.
These tips can help you feel less itchy:
Keep cool because heat and sweat will make you itch more. You might want to put a cool, wet washcloth on the really bad areas.
Trim your fingernails, so if you do scratch, you won't tear your skin.
Soak in a lukewarm bath. Adding some oatmeal to your bath water can help relieve the itching.
Have your mom or dad help you apply calamine lotion, which soothes itching.
Don't Scratch
Scratching the blisters can tear your skin and leave scars. Scratching also can let germs in, and the blisters could get infected. If your fever goes higher and an area of your skin gets really red, warm, and painful, tell an adult right away. You'll need to see a doctor because you could have a skin infection.
While you have the chickenpox, a pain reliever like acetaminophen might help you feel better, but let your parents help you with this.
Do not take aspirin, because it can cause a rare but serious illness in kids called Reye syndrome. Medicines and creams that may stop the itch can also be helpful.
It doesn't usually happen, but let your parents know if you feel especially bad. Sometimes, chickenpox leads to other, more serious illnesses.
Most kids don't have any major problems and get better in a week or two. And when all the blisters have scabs, you're not contagious anymore and you can go back to school! In a few days, the scabs will fall off. And once you've had chickenpox, it's unlikely you'll ever get it again.
Get a Shot, Avoid the Dots!
Not long ago, 3 million people got chickenpox each year in the United States. But now that kids receive the shot, fewer and fewer people get chickenpox.
Have you had the chickenpox vaccine? You might not remember because it's often given at age 1. But you can get it when you're older, too. Ask your mom or dad if you've had yours. You'll be glad that you did if chickenpox starts making its way around your school!
Viral hemorrhagic fevers (VHFs) are a group of illnesses caused by four families of viruses. These include the Ebola and Marburg, Lassa fever, and yellow fever viruses. VHFs have common features: they affect many organs, they damage the blood vessels, and they affect the body's ability to regulate itself. Some VHFs cause mild disease, but some, like Ebola or Marburg, cause severe disease and death.
VHFs are found around the world. Specific diseases are usually limited to areas where the animals that carry them live. For example, Lassa fever is limited to rural areas of West Africa where rats and mice carry the virus.
The risk for travelers is low, but you should avoid visiting areas where there are disease outbreaks. Because there are no effective treatments for some of these viral infections, there is concern about their use in bioterrorism.
Definition
Pneumonia is an infection that inflames the air sacs in one or both lungs. The air sacs may fill with fluid or pus, causing cough with phlegm or pus, fever, chills and difficulty breathing.
A variety of organisms, including bacteria, viruses and fungi, can cause pneumonia.
Pneumonia can range in seriousness from mild to life-threatening. It is most serious for infants and young children, people older than age 65, and people with underlying health problems or weakened immune systems.
Antibiotics and antiviral medications can treat many common forms of pneumonia.
Symptoms
The signs and symptoms of pneumonia vary from mild to severe, depending upon factors such as the type of germ causing the infection and your age and overall health. Mild signs and symptoms often are similar to those of a cold or flu, but they last longer.
Newborns and infants may not show any sign of the infection. Or they may vomit, have a fever and cough, appear restless or tired and without energy, or have difficulty breathing and eating.
Older people who have pneumonia sometimes have sudden changes in mental awareness.
WHEN TO SEE A DOCTOR See your doctor if you have difficulty breathing, chest pain, persistent fever of 39 C or higher or persistent cough, especially if you are coughing up pus.
It's especially important to see a doctor if:
A child with signs and symptoms is younger than age 2
You are older than age 65
You have an underlying health condition or weakened immune system
You're having chemotherapy or taking medication that suppresses your immune system
For some older adults and people with heart failure or lung ailments, pneumonia can quickly become a life-threatening condition.
Causes
Pneumonia has many possible causes. The most common are bacteria and viruses in the air we breathe. Your body usually prevents these germs from infecting your lungs. But sometimes these germs can overpower your immune system, even if your health is generally good.
Pneumonia is classified according to the types of germs that cause it, and where you acquired the infection.
Community-acquired pneumonia Community-acquired pneumonia is the most common type of pneumonia. It occurs outside of hospitals and other health care facilities, and may be caused by:
Bacteria, such as Streptococcus pneumoniae. Bacterial community-acquired pneumonia can occur on its own or after you have a cold or respiratory flu. This type of pneumonia often affects one area (lobe) of the lung, a condition called lobar pneumonia.
Bacteria-like organisms, such as Mycoplasma pneumoniae, which typically produce milder signs and symptoms than do other types of pneumonia. "Walking pneumonia," a term used to describe pneumonia that isn't severe enough to require bed rest, may result from Mycoplasma pneumoniae.
Viruses, including some that are the same type of viruses that cause colds and flu. Viruses are the most common cause of pneumonia in children younger than 2 years. Viral pneumonia is usually mild. But viral pneumonia caused by certain influenza viruses, such as sudden acute respiratory syndrome (SARS), can become very serious.
Fungi, which can be found in soil and in bird droppings. This type of pneumonia is most common in people with an underlying health problem or weakened immune system and in people who have inhaled a large dose of the organisms.
Hospital-acquired pneumonia
Hospital-acquired pneumonia is a bacterial infection that occurs in people 48 hours or more after being hospitalized for another condition. Hospital-acquired pneumonia can be serious because the bacteria causing it may be more resistant to antibiotics.
People who are on a breathing machine (ventilator), often used in intensive care units, are at higher risk of this type of pneumonia.
Health care-acquired pneumonia Health care-acquired pneumonia is a bacterial infection that occurs in people who are living in long-term care facilities or have been treated in outpatient clinics, including kidney dialysis centers. Like hospital-acquired pneumonia, health care-acquired pneumonia can be caused by bacteria more resistant to antibiotics.
Aspiration pneumonia Aspiration pneumonia occurs when you inhale food, drink, vomit or saliva into your lungs. This aspiration may happen if something disturbs your normal gag reflex, such as a brain injury, swallowing problem, or excessive use of alcohol or drugs.
Risk factors
Pneumonia can affect anyone. But the two age groups at highest risk are:
Infants and children younger than age 2 years, because their immune systems are still developing
People older than age 65
Other risk factors include:
Certain chronic diseases, such as asthma, chronic obstructive pulmonary disease and heart disease
Weakened or suppressed immune system, due to factors such as HIV/AIDS, organ transplant, chemotherapy for cancer or long-term steroid use
Smoking, which damages your body's natural defenses against the bacteria and viruses that cause pneumonia
Being placed on a ventilator while hospitalized
Complications
Often, people who have pneumonia can be treated successfully with medication. But some people, especially those in high-risk groups, may experience complications, including:
Bacteria in the bloodstream (bacteremia). Bacteria that enter the bloodstream from your lungs can spread the infection to other organs, potentially causing organ failure.
Lung abscess. An abscess occurs if pus forms in a cavity in the lung. An abscess is usually treated with antibiotics. Sometimes, surgery or drainage with a long needle or tube placed into the abscess is needed to remove the pus.
Fluid accumulation around your lungs (pleural effusion). Pneumonia may cause fluid to build up in the thin space between layers of tissue that line the lungs and chest cavity (pleura). If the fluid becomes infected, you may need to have it drained through a chest tube or removed with surgery.
Difficulty breathing. If your pneumonia is severe or you have chronic underlying lung diseases, you may have trouble breathing in enough oxygen. You may need to be hospitalized and use a mechanical ventilator while your lung heals.
Tests and diagnosis
Your doctor will start by asking about your medical history and doing a physical exam, including listening to your lungs with a stethoscope to check for abnormal bubbling or crackling sounds that indicate the presence of thick liquid.
If pneumonia is suspected, your doctor may recommend:
Chest X-rays, to confirm the presence of pneumonia and determine the extent and location of the infection.
Blood tests, to confirm the presence of infection and to try to identify the type of organism causing the infection. Precise identification occurs in only about half of people with pneumonia.
Pulse oximetry, to measure the oxygen level in your blood. Pneumonia can prevent your lungs from moving enough oxygen into your bloodstream.
Sputum test. A sample of fluid from yours lungs (sputum) is taken after a deep cough, and analyzed to pinpoint the type of infection.
If you are older than age 65, are in the hospital or have serious symptoms or an underlying health condition, your doctor may recommend:
Pleural fluid culture. A fluid sample is taken from the pleural area and analyzed to help determine the type of infection.
Bronchoscopy. A thin, flexible tube with a camera is inserted down your throat and through your airways to check whether something is blocking the airways or whether something else is contributing to your pneumonia.
If your pneumonia isn't clearing as quickly as expected, your doctor may recommend a chest CT scan to obtain a more detailed image of your lungs.
Treatments and drugs
Treatment for pneumonia involves curing the infection and preventing any complications.
People who have community-acquired pneumonia usually can be treated at home with medication. Although your symptoms may ease in a few days or weeks, tiredness can persist for a month or more.
Your doctor will likely recommend a follow-up chest X-ray to check that the infection is clearing. It may be safe to stop treatment even if your X-ray isn't completely normal. Only about half of chest X-rays in people with community-acquired pneumonia are normal after 28 days of treatment.
Specific treatments depend on the type and severity of your pneumonia, and your age and overall health. The options include:
Antibiotics, to treat bacterial pneumonia. It may take time to identify the type of bacteria causing your pneumonia and to choose the best antibiotic to treat it. Symptoms often improve within three days, although improvement usually takes twice as long in smokers. If your symptoms don't improve, your doctor may recommend a different antibiotic.
Antiviral medications, to treat viral pneumonia. Symptoms generally improve in one to three weeks.
Fever reducers, such as aspirin or ibuprofen.
Cough medicine, to calm your cough so you can rest. Because coughing helps loosen and move fluid from your lungs, it's a good idea not to eliminate your cough completely.
If you need to be placed on a ventilator or your symptoms are severe, you may need to be admitted to an intensive care unit.
Children may be hospitalized if they:
Are younger than age 3 months
Are excessively sleepy
Have trouble breathing
Have low blood oxygen levels
Appear dehydrated
Have a lower than normal temperature
Lifestyle and home remedies
To help you recover more quickly and decrease your risk of complications:
Get plenty of rest. Even when you start to feel better, be careful not to overdo it.
Stay home from school or work until after your temperature returns to normal and you stop coughing up mucus. Because pneumonia can recur, it's better not to return to a full workload until you're sure you're well. Ask your doctor if you're not sure.
Drink plenty of fluids, especially water, to help loosen mucus in your lungs.
Take the entire course of any prescribed medications. If you stop medication too soon, your lungs may continue to harbor bacteria that can multiply and cause your pneumonia to recur.
Prevention
To help prevent pneumonia:
Get a seasonal flu shot. The influenza virus can be a direct cause of viral pneumonia. Bacterial pneumonia is also a common complication of the flu. A yearly flu shot provides significant protection.
Link to the Vaccination
Get a pneumonia vaccination. Doctors recommend a one-time vaccine against Streptococcus pneumoniae bacteria (pneumococcus) for everyone older than age 65, as well as for people of any age residing in nursing homes and long-term care facilities, and for smokers. The vaccine is especially recommended for anyone at high risk of pneumococcal pneumonia. Some doctors recommend a booster shot five years after the first dose.
Have your child vaccinated. Doctors recommend a different pneumonia vaccine for all children younger than age 2 and for children ages 2 to 5 years who are at particular risk of pneumococcal disease. Children who attend a group day care center should also get the vaccine. Doctors also recommend seasonal flu shots for children older than six months.
Practice good hygiene. To protect yourself against ordinary respiratory infections that sometimes lead to pneumonia, wash your hands regularly or use an alcohol-based hand sanitizer.
Don't smoke. Smoking damages your lungs' natural defenses against respiratory infections.
Stay rested and fit. Proper rest, a healthy diet and moderate exercise can help keep your immune system strong.
Set an example. Stay home when you're sick. When you're in public and have a cold, catch your coughs and sneezes in the inner crook of your elbow.
Parainfluenza refers to a group of viruses that lead to upper and lower respiratory infections.
Causes
There are four types of parainfluenza virus, all of which can cause upper respiratory infections or lower respiratory infections (pneumonia) in adults and children. The virus can cause croup, bronchiolitis, bronchitis and certain types of pneumonia.
The exact number of cases of parainfluenza is unknown but suspected to be very high. Sometimes the viruses cause only a runny nose and other symptoms that may be diagnosed as a simple cold rather than parainfluenza.
Infections are most common in fall and winter. Parainfluenza infections are most severe in infants and become less severe with age. By school age, most children have been exposed to parainfluenza virus. Most adults have antibodies against parainfluenza although they can get repeat infections.
Symptoms
Symptoms vary depending on the type of infection. Cold-like symptoms consisting of a runny nose and mild cough are common. Life-threatening respiratory symptoms can be seen in young infants with bronchiolitis and those with weakened immune systems.
A physical exam may show sinus tenderness, swollen glands, and a red throat. The doctor will listen to the lungs and chest with a stethoscope. Abnormal sounds, such as crackling or wheezing, may be heard.
Tests that may be done include:
Arterial blood gases
Chest x-ray
CT scan of the chest
Complete blood count (CBC)
Swab of nose for rapid viral test
Treatment
There is no specific treatment for the viral infection. Specific treatments are available for the symptoms of croup and bronchiolitis to make breathing easier.
Outlook (Prognosis)
Most infections in adults and older children are mild and recovery takes place without treatment, unless the person is very old or has an abnormal immune system. Medical intervention may be necessary if breathing difficulties develop.
Possible Complications
Secondary bacterial infections are the most common complication. Airway obstruction in croup and bronchiolitis can be severe, even life-threatening.
When to Contact a Medical Professional
Call your health care provider if you or your child develops croup, wheezing or any other type of breathing difficulty. Contact your health care provider if a child under 18 months develops any type of upper respiratory symptoms.
Prevention
There are no vaccines available for parainfluenza. Avoiding crowds to limit exposure during peak outbreaks may decrease the likelihood of infection.
Limiting exposure to daycare centers and nurseries may delay infection until the child is older.
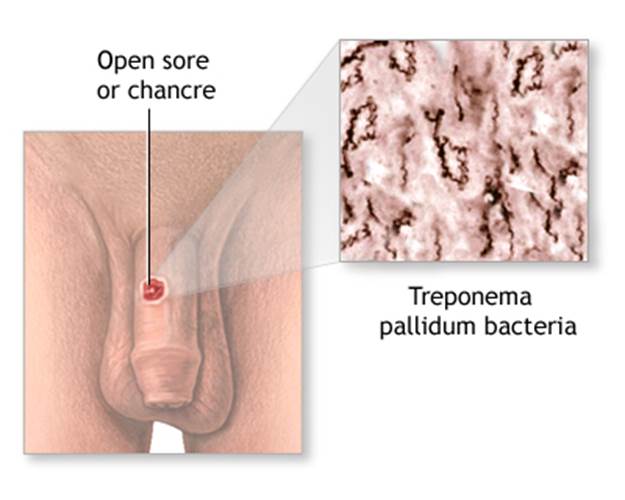
Syphilis is bacteria infection that is most often spread through sexual contact.
Causes
Syphilis is a sexually transmitted, infectious disease caused by the spirochete Treponema pallidum. This bacterium causes infection when it gets into broken skin or mucus membranes, usually of the genitals. Syphilis is most often transmitted through sexual contact, although it also can be transmitted in other ways.
Syphilis occurs worldwide. Syphilis is more common in urban areas, and the number of cases is rising fastest in men who have sex with men. Young adults ages 15 - 25 are the highest-risk population. People have no natural resistance to syphilis.
Because people may be unaware that they are infected with syphilis, many states require tests for syphilis before marriage. All pregnant women who receive prenatal care should be screened for syphilis to prevent the infection from passing to their newborn (congenital syphilis).
Syphilis has three stages:
Primary syphilis
Secondary syphilis
Tertiary syphilis (the late phase of the illness)
Secondary syphilis, tertiary syphilis, and congenital syphilis are not seen as often in the United States as they were in the past because of the availability of:
Blood tests to screen for syphillis bacteria (RPR or VDRL)-- if positive, one of the following tests will be needed to confirm the diagnosis:
FTA-ABS (fluorescent treponemal antibody test)
MHA-TP
Spinal tap, and examination of spinal fluid
Treatment
Syphilis can be treated with antibiotics, such as penicillin G benzathine, doxycycline, or tetracycline (for patients who are allergic to penicillin). Length of treatment depends on how severe the syphilis is, and factors such as the patient's overall health.
For treating syphilis during pregnancy, penicillin is the drug of choice. Tetracycline cannot be used because it is dangerous to the unborn baby. Erythromycin may not prevent congenital syphilis in the baby. People who are allergic to penicillin should ideally be desensitized to it, and then treated with penicillin.
Several hours after getting treatment for the early stages of syphilis, people may experience Jarish-Herxheimer reaction. This is caused by an immune reaction to the breakdown products of the infection.
Follow-up blood tests must be done at 3, 6, 12, and 24 months to ensure that the infection is gone. Avoid sexual contact when the chancre is present, and use condoms until two follow-up tests have indicated that the infection has been cured.
All sexual partners of the person with syphilis should also be treated. Syphilis is extremely contagious in the primary and secondary stages.
Outlook (Prognosis)
Syphilis can be cured if it is diagnosed early and completely treated.
Secondary syphilis can be cured if it is diagnosed early and treated effectively. Although it usually goes away within weeks, in some cases it may last for up to 1 year. Without treatment, up to one-third of patients will have late complications of syphilis.
Late syphilis may be permanently disabling, and it may lead to death.
In addition, untreated secondary syphilis during pregnancy may spread the disease to the developing baby. This is called congenital syphilis.
When to Contact a Medical Professional
Call for an appointment with your health care provider if you have symptoms of syphilis.
If you have had intimate contact with a person who has syphilis or any other STI, or have engaged in any high-risk sexual practices, including having multiple or unknown partners or using intravenous drugs, contact your doctor or nurse, or get screened in an STI clinic.
Prevention
If you are sexually active, practice safe sex and always use a condom.
All pregnant women should be screened for syphilis.
Alternative Names
Primary syphilis; Secondary syphilis; Late syphilis; Tertiary syphilis
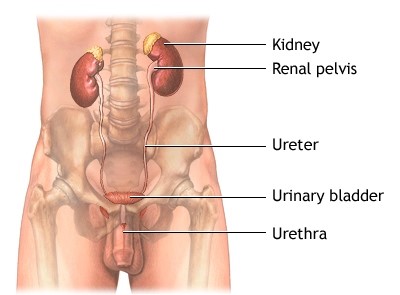
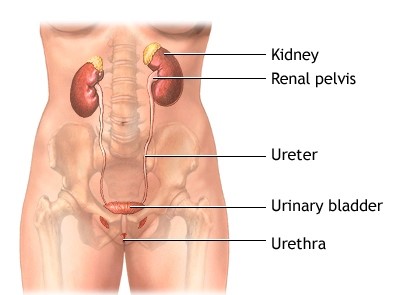
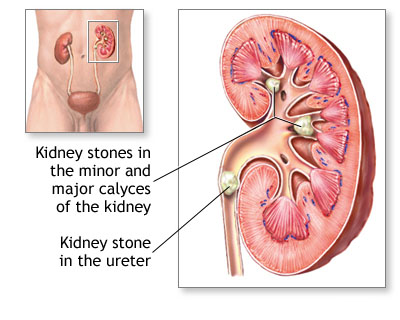
The urinary tract is the body’s drainage system for removing wastes and extra water. The urinary tract includes two kidneys, two ureters, a bladder, and a urethra. The kidneys are two bean-shaped organs, each about the size of a fist. They are located near the middle of the back, just below the rib cage, one on each side of the spine. Every day, the two kidneys process about 200 quarts of blood to produce about 1 to 2 quarts of urine, composed of wastes and extra water. Children produce less urine than adults. The amount produced depends on their age. The urine flows from the kidneys to the bladder through tubes called the ureters. The bladder stores urine until releasing it through urination. When the bladder empties, urine flows out of the body through a tube called the urethra at the bottom of the bladder.
Pyelonephritis is caused by a bacterium or virus infecting the kidneys. Though many bacteria and viruses can cause pyelonephritis, the bacterium Escherichia coli is often the cause. Bacteria and viruses can move to the kidneys from the bladder or can be carried through the bloodstream from other parts of the body. A UTI in the bladder that does not move to the kidneys is called cystitis.
People most at risk for pyelonephritis are those who have a bladder infection and those with a structural, or anatomic, problem in the urinary tract. Urine normally flows only in one direction—from the kidneys to the bladder. However, the flow of urine may be blocked in people with a structural defect of the urinary tract, a kidney stone, or an enlarged prostate—the walnut-shaped gland in men that surrounds the urethra at the neck of the bladder and supplies fluid that goes into semen. Urine can also back up, or reflux, into one or both kidneys. This problem, which is called vesicoureteral reflux (VUR), happens when the valve mechanism that normally prevents backward flow of urine is not working properly. VUR is most commonly diagnosed during childhood. Pregnant women and people with diabetes or a weakened immune system are also at increased risk of pyelonephritis.
Children younger than 2 years old may only have a high fever without symptoms related to the urinary tract. Older people may not have any symptoms related to the urinary tract either; instead, they may exhibit confusion, disordered speech, or hallucinations.
Most people with pyelonephritis do not have complications if appropriately treated with bacteria-fighting medications called antibiotics.
In rare cases, pyelonephritis may cause permanent kidney scars, which can lead to chronic kidney disease, high blood pressure, and kidney failure. These problems usually occur in people with a structural problem in the urinary tract, kidney disease from other causes, or repeated episodes of pyelonephritis.
Infection in the kidneys may spread to the bloodstream—a serious condition called sepsis—though this is also uncommon.
The tests used to diagnose pyelonephritis depend on the patient’s age, gender, and response to treatment and include the following:
Urinalysis. Urinalysis is testing of a urine sample. The urine sample is collected in a special container in a health care provider’s office or commercial facility and can be tested in the same location or sent to a lab for analysis. The presence of white blood cells and bacteria in the urine indicate infection.
Urine culture. A urine culture is performed by placing part of a urine sample in a tube or dish with a substance that encourages any bacteria present to grow. The urine sample is collected in a special container in a health care provider’s office or commercial facility and sent to a lab for culture. Once the bacteria have multiplied, which usually takes 1 to 3 days, they can be identified. The health care provider can then determine the best treatment.
Ultrasound. Ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. The procedure is performed in a health care provider’s office, outpatient center, or hospital by a specially trained technician, and the images are interpreted by a radiologist—a doctor who specializes in medical imaging; anesthesia is not needed. The images can show obstructions in the urinary tract. Ultrasound is often used for people who do not respond to treatment within 72 hours.
Computerized tomography (CT) scan. CT scans use a combination of x rays and computer technology to create three-dimensional (3-D) images. A CT scan may include the injection of a special dye, called contrast medium. CT scans require the person to lie on a table that slides into a tunnel-shaped device where the x rays are taken. The procedure is performed in an outpatient center or hospital by an x-ray technician, and the images are interpreted by a radiologist. Anesthesia is not needed. CT scans can show obstructions in the urinary tract. The test is often used for people who do not respond to treatment within 72 hours.
Voiding cystourethrogram (VCUG). A VCUG is an x-ray image of the bladder and urethra taken while the bladder is full and during urination, also called voiding. The procedure is performed in an outpatient center or hospital by an x-ray technician supervised by a radiologist, who then interprets the images. Anesthesia is not needed, but sedation may be used for some people. The bladder and urethra are filled with contrast medium to make the structures clearly visible on the x-ray images. The x-ray machine captures images of the contrast medium while the bladder is full and when the person urinates. This test can show abnormalities of the inside of the urethra and bladder and is usually used to detect VUR in children.
Digital rectal examination (DRE). A DRE is a physical exam of the prostate that is performed in the health care provider’s office. Anesthesia is not needed. To perform the exam, the health care provider asks the person to bend over a table or lie on his side while holding his knees close to his chest. The health care provider slides a gloved, lubricated finger into the rectum and feels the part of the prostate that lies in front of the rectum. Men with suspected pyelonephritis may have a DRE to determine whether a swollen prostate may be obstructing the neck of the bladder.
Dimercaptosuccinic acid (DMSA) scintigraphy. DMSA scintigraphy is an imaging technique that relies on the detection of small amounts of radiation after injection of radioactive material. Because the dose of radioactive material is small, the risk of causing damage to cells is low. The procedure is performed in an outpatient center or hospital by a specially trained technician, and the images are interpreted by a radiologist. Anesthesia is not needed. Radioactive material is injected into a vein in the person’s arm and travels through the body to the kidneys. Special cameras and computers are used to create images of the radioactive material as it passes through the kidneys. The radioactive material makes the parts of the kidney that are infected or scarred stand out on the image. DMSA scintigraphy is used to show the severity of kidney infection or kidney damage, such as scarring.
Pyelonephritis is treated with antibiotics, which may need to be taken for several weeks. While a urine sample is sent to a lab for culture, the health care provider may begin treatment with an antibiotic that fights the most common types of bacteria. Once culture results are known and the bacteria is clearly identified, the health care provider may switch the antibiotic to one that more effectively targets the bacteria. Antibiotics may be given through a vein, orally, or both. Urinary tract obstructions are often treated with surgery.
Severely ill patients may be hospitalized and limited to bed rest until they can take the fluids and medications they need on their own. Fluids and medications may be given intravenously during this time.
In adults, repeat urine cultures should be performed after treatment has ended to make sure the infection does not recur. If a repeat test shows infection, another 14-day course of antibiotics is prescribed; if infection recurs again, antibiotics are prescribed for 6 weeks.
Pyelonephritis is a type of urinary tract infection that affects one or both kidneys.
Pyelonephritis is caused by a bacterium or virus infecting the kidneys. Though many bacteria and viruses can cause pyelonephritis, the bacterium Escherichia coli is often the cause. Bacteria and viruses can move to the kidneys from the bladder or can be carried through the bloodstream from other parts of the body.
Symptoms of pyelonephritis can vary depending on a person’s age and may include the following:
Children younger than 2 years old may only have a high fever without symptoms related to the urinary tract. Older people may not have any symptoms related to the urinary tract either; instead, they may exhibit confusion, disordered speech, or hallucinations.
Most people with pyelonephritis do not have complications if appropriately treated with bacteria-fighting medications called antibiotics.
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you? Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses.
A kidney stone is a solid mass made up of tiny crystals. One or more stones can be in the kidney or ureter at the same time.
Kidney stones result when urine becomes too concentrated and substances in the urine crystalize to form stones. Symptoms arise when the stones begin to move down the ureter causing intense pain. Kidney stones may form in the pelvis or calyces of the kidney or in the ureter.
Kidney stones are common. Some types run in families. They often occur in premature infants.
There are different types of kidney stones. The cause of the problem depends on the type of stone.
Stones can form when urine contains too much of certain substances that form crystals. These crystals can develop into stones over weeks or months.
Calcium stones are most common. They are most likely to occur in men between ages 20 - 30. Calcium can combine with other substances to form the stone.
Oxalate is the most common of these. Oxalate is present in certain foods such as spinach. It's also found in vitamin C supplements. Diseases of the small intestine increase your risk of these stones.
Calcium stones can also form from combining with phosphate or carbonate.
Other types of stones include:
Cystine stones can form in people who have cystinuria. This disorder runs in families. It affects both men and women.
Struvite stones are mostly found in women who have a urinary tract infection. These stones can grow very large and can block the kidney, ureter, or bladder.
Uric acid stones are more common in men than in women. They can occur with gout or chemotherapy.
Other substances such as certain medicines also can form stones.
The biggest risk factor for kidney stones is not drinking enough fluids. Kidney stones are more likely to occur if you make less than 1 liter of urine a day.
You may not have symptoms until the stones move down the tubes (ureters) through which urine empties into your bladder. When this happens, the stones can block the flow of urine out of the kidneys.
The main symptom is severe pain that starts suddenly and may go away suddenly:
Pain may be felt in the belly area or side of the back.
Treatment depends on the type of stone and the severity of your symptoms.
Kidney stones that are small usually pass through your system on their own.
Your urine should be strained so the stone can be saved and tested.
Drink at least 6 - 8 glasses of water per day to produce a large amount of urine. This will help the stone pass.
Pain can very bad. Over the counter pain medicines (e.g. ibuprofen, naproxen), either alone or along with narcotics, can be very effective.
Some people with severe pain from kidney stones need to stay in the hospital. You may need to get fluids through a vein.
For some types of stones, your doctor may prescribe medicine to prevent stones from forming or help break down and remove the material that is causing the stone. These medicines can include:
The stone is blocking urine flow and causing an infection or kidney damage.
The pain cannot be controlled.
Today, most treatments are much less invasive than in the past.
Lithotripsy is used to remove stones slightly smaller than a half an inch that are located in the kidney or ureter. It uses sound or shock waves to break up stones. Then, the stone fragments leave the body in the urine. It is also called extracorporeal shock-wave lithotripsy or ESWL.
Procedures performed by passing a special instrument through a small surgical cut in your skin and into your kidney or ureters are used for large stones in or near the kidney, or when the kidneys or surrounding areas are incorrectly formed. The stone is removed with a tube (endoscope).
Ureteroscopy may be used for stones in the lower urinary tract.
Rarely, open surgery (nephrolithotomy) may be needed if other methods do not work or are not possible.
Talk to your doctor about what treatment options may work for you.
Call your health care provider if you have symptoms of a kidney stone.
Very bad pain in your back or side that will not go away
Blood in your urine
Fever and chills
Vomiting
Urine that smells bad or looks cloudy
A burning feeling when you urinate
If you have been diagnosed with blockage from a stone, passage must be confirmed either by capture in a strainer during urination or by follow-up x-ray.
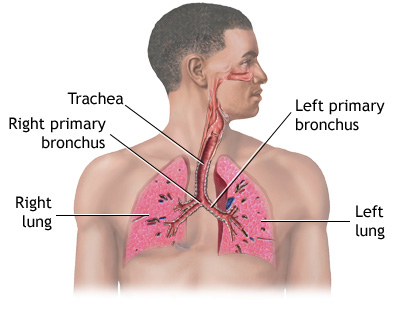
Tracheitis is a bacterial infection of the windpipe (trachea).
Causes
Bacterial tracheitis is most often caused by the bacteria Staphylococcus aureus. It often follows a recent viral upper respiratory infection. It affects mostly young children, possibly because their small trachea is easily blocked by swelling.
The health care provider will perform a physical exam and listen to the child's lungs. The muscles between the ribs may pull in as the child tries to breathe. This is called intercostal retractions.
Tests that may be done to diagnose this condition include:
Tracheitis is an emergency medical condition. Go to the emergency room right away if your child has had a recent upper respiratory infection and suddenly has a high fever, a cough that gets worse, or trouble breathing.
Alternative Names
Bacterial tracheitis; Acute bacterial tracheitis
Pilonidal dimple is a condition that can occur anywhere along the crease between the buttocks, which runs from the bone at the bottom of the spine (sacrum) to the anus.
Pilonidal dimple may appear as:
A pilonidal abscess, in which the hair follicle becomes infected and pus collects in the fat tissue
A pilonidal cyst, in which a cyst or hole forms if there has been an abscess for a long time
A pilonidal sinus, in which a tract grows under the skin or deeper from the hair follicle
A small pit or pore in the skin that contains dark spots or hair
SYMPTOMS
Pus may drain to a small pit in the skin
Tenderness over the area after you are active or sit for a period of time
Warm, tender, swollen area near the tailbone
Fever (rare)
There may be no symptoms other than a small dent (pit) in the skin in the crease between the buttocks.
CAUSES
The cause of pilonidal disease is not clear. It is thought to be caused by hair growing into the skin in the crease between the buttocks.
This problem is more likely to occur in people who:
Are obese
Experienced trauma or irritation in the area
Have excess body hair
Sit for long periods of time
Wear tight clothing
HOME CARE
It may help to keep the area clean and dry and remove hair regularly to prevent infection.
WHEN TO CONTACT A DOCTOR
Call your health care provider if you notice any of the following around the pilonidal cyst:
Pilonidal disease that causes no symptoms does not need to be treated.
A pilonidal abscess may be opened, drained, and packed with gauze. Antibiotics may be used if there is an infection spreading in the skin or you also have another, more severe illness.
Mycoplasma pneumonia is an infection of the lungs by the bacteria Mycoplasma pneumoniae (M. pneumoniae).
Mycoplasma pneumonia usually affects people younger than 40.
People at highest risk for mycoplasma pneumonia include those living or working in crowded areas such as schools and homeless shelters, although many people with it have no identifiable risk factor.
The symptoms are generally mild and appear over a period of 1 to 3 weeks. They may become more severe in some people.
Common symptoms include the following:
Chest pain
Chills
Cough, usually dry and not bloody
Excessive sweating
Fever (may be high)
Headache
Sore throat
Less common symptoms include:
Ear pain
Eye pain or soreness
Muscle aches and joint stiffness
Neck lump
Rapid breathing
Skin lesions or rash
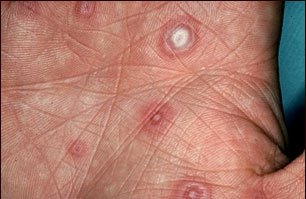
Erythema multiforme lesions are often referred to as target lesions because of the concentric rings the lesions produce. The "target" appearance is well demonstrated in this photograph.
Persons with suspected pneumonia should have a complete medical evaluation, including a thorough physical exam and a chest x-ray -- especially because the physical exam may not always be able to tell pneumonia apart from acute bronchitis or other respiratory infections.
Depending on the severity of illness, other tests may be done, including:
Complete blood count (CBC)
Blood cultures
Blood tests for signs of mycoplasma infection
Bronchoscopy
CT scan of the chest
Open lung biopsy (only done in very serious illnesses when the diagnosis cannot be made from other sources)
Antibiotics that work against Mycoplasma include macrolides, fluroquinolones, and tetracyclines. You can take these steps at home:
Control your fever with aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs, such as ibuprofen or naproxen), or acetaminophen. DO NOT give aspirin to children.
Do not take cough medicines without first talking to your doctor. Cough medicines may make it harder for your body to cough up the extra sputum.
Drink plenty of fluids to help loosen secretions and bring up phlegm.
Get a lot of rest. Have someone else do household chores.
Most people recover completely even without antibiotics, although antibiotics may speed recovery. In untreated adults, cough and weakness can persist for up to a month. The disease can be more serious in the elderly and those with a weakened immune system.
Call for an appointment with your health care provider if you develop a fever, cough, or shortness of breath. While there are numerous causes for these symptoms, you will need to be checked for pneumonia.
Also, call if you have been diagnosed with this type of pneumonia and your symptoms become worse.
Azithromycin can reduce the risk of developing mycoplasma pneumonia in close contacts of patients with the disease. However, this is not often used, and avoiding people who have the infection may also help reduce yourrisk.
Infants, and persons in poor health, especially those with weakened immune systems due to HIV, organ transplants, or other conditions should avoid contact with people who have mycoplasma pneumonia.