Ауруға көбінесе, балалар ұшырайды. Тек ауру адамнан жұқтыруға болады.
Адам ішекқұртты олардың жетілген жұмыртқасы тағаммен аузына немесе шаңмен ішіне түскенде жұқтырады. Энтеробиозға ұшыраған адам саусағы ластанғанда өзіне-өзі жұқтырады (науқастар айналшықтың маңындағы теріні қасиды, себебі күшті қышу мазайлайды).
Науқастың терісінде ішекқұрттық аналығы салған жұмыртқалар 4-6 сағаттан кейін жетіледі де адам жұқпалы болады. жұмыртқалар төсекке және науқастың іш киіміне, үйдегі және жұмыс орнындағы заттарға түседі.
Энтеробиозды анықтау үшін Грэхем әдісін қолданып, зерттеу қажет, ол үшін жабысқақ лента қолданылады. ішекқұрт жұмыртқаларын тырнақ астынан алған жұғындыдан да табуға болады. ішекқұрттардың қозғалатын ересек аналығын науқастың нәжісінің бетінен көруге болады.
Конъюнктива бактериялардың және басқа тітіркендіргіштердің әрекетіне ұшырайды. Көз жасы бактерияларды шайып, конъюнктиваны қорғауға көмектеседі. Сондай-ақ, көз жасында ақуыздар және бактерияларды жоятын антиденелер болады.
Конъюнктивиттің пайда болуының көптеген себептері бар. Вирустар аса кең таралған себебін құрайды. Вирустық конъюнктивитті «қызғылт көз» деп те атайды. «Қызғылт көз» балалардың арасында жеңіл тарауы мүмкін.
Контактілік линзаларды қолдану (әсіресе, ұзақ уақыт бойы қолдануға арналған линзалар)
Жаңа туған сәбилер босану жолдарында бактериялармен жұқпалануы мүмкін. Бұл жағдай жаңа туған сәбилердің офтальмиясы аталады, көруді сақтау үшін бұл дереу емделуі тиіс.
Аллергиялық конъюнктивит аллергияны емдеу кезінде жазылып кетуі мүмкін. Аллергияны туындатқан себебімен қатынас жойылса, өз бетінше жазылып кетуі мүмкін. Суық компресс қою аллергиялық конъюнктивитті басуға көмектесуі мүмкін.
Антибиотикпен емдеу, көбінесе, көз тамшылары, бактериалдық конъюнктивитте тиімді.
Вирустық конъюнктивит өз бетінше өтеді.
Көптеген дәрігерлер «қызғылт көз» кезінде бактериалдық конъюнктивиттің алдын алу үшін жеңіл антибактериалдық көз тамшыларын тағайындайды.
Сіз вирустық немесе бактериалдық конъюнктивит кезінде жылы компресс қолдану арқылы жайсыздықты баса аласыз (көзге жабық күйінде жылы суға малынған матаны басу қажет).
Себореялық дерматит – терінің жиі кездесетін, қабыну ауруы. Бұл кезде шаштың түбіндегі, бет пен құлақтың май безі жақсы дамыған бөліктерінде ақ-сары тұстары болады. олар өзгермеген немесе қызармаған тұста пайда болуы мүмкін.
«Бесік телпегі» - сәбилерде себореялық дерматит кезіндегі бастың терісінің зақымдануын сипаттайтын термин.
Себореялық дерматиттің нақты себебі белгісіз. Дәрігерлердің ойынша, ол бірнеше себептің бірігуінен болуы мүмкін, гормоналдық үйлесімнің бұзылуын, иммундық жүйенің әлсіреуін, қоректік заттектердің жеткіліксіздігін, немесе жүйке жүйесінің ауруларын қоса.
Malassezia зеңдерінен пайда болатын тітіркеніс те осы жағдайға әкелуі мүмкін. Себореялық дерматит тұқым қуалауы мүмкін.
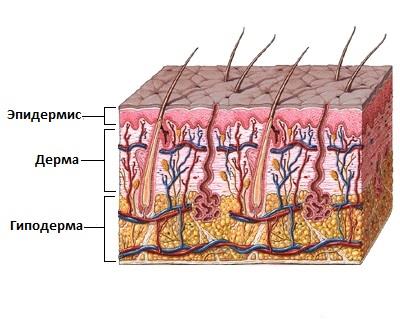
Терінің қабаттары
Қауіп факторлары:
Күйзеліс немесе шаршау
Экстремалдық ауа райы
Майлы тері немесе терідегі безеулер
Кейбір сусабындар немесе теріге күтім жасау құралы
Спирт құрамдас лосьондар қолдану
Семіздік
Неврологиялық аурулар, оның ішінде, бассүйек-ми жарақаты, Паркинсон ауруы немесе инсульт
Себореялық дерматит дененің әр бөлігінде пайда болуы мүмкін. Әдетте, ол терінің май безі жақсы дамыған тұстарында пайда болады. Көбінесе, бұл бастың, қабақтың терісі, мұрын-ерін қыртысы, құлақ артындағы, сыртқы құлақтағы тұстар, сондай-ақ, кеуде қуысы.
Себореялық дерматиттің симптомдары:
• Терінің зақымдануы
• Терінің үлкен аумағындағы түйіндақтар
• Терінің майлы бөліктері
• Теріде ақ, қабыршақтанған, сары, майлы бөліктердің пайда болуы
Қабыршақтану мен құрғақтықты қайызғаққа арналған арнайы сусабынның көмегімен емдеуге болады. оларды дәріханада дәрігердің рецептінісіз сатып алуға болады. жапсырмасында себореялық дерматитті емдейді деп жазылған сусабынды іздеңіз. Олардың құрамында салицил қышқылы, таскөмір шайыры, мырыш, резорцин, кетоконазол немесе селен сульфиді секілді құрамбөліктер болады. сусабындарды нұсқаулығында көрсетілуіне сәйкес қолданыңыз.
Аурудың ауыр өтуінде дәрігер селен сульфидінің, кетоконазол немесе кортикостероидтардың мөлшері жоғары сусабынды немесе лосьонды қолдануды тағайындауы мүмкін. Сондай-ақ, құрамында иммунитетті ынталандырғыш болатын крем ұсынылуы мүмкін. Бұл дәрі иммундық жүйенің жұмысын басуға қабілетті, осылайша, қабынуды азайтады.
Күн сәулесінің әсер етуінде себореялық дерматиттің барысы жақсарады деп саналады. Кейбір адамдар жазда жағдай жақсаратындығын айтады, әсіресе, белсенді демалыстан кейін.
Дәрігерден кеңес алыңыз, егер себореялық дерматиттің симптомдары үй жағдайында емдеуге және дәрігердің рецептінсіз босатылатын дәрі препараттарын қабылдауға серпін бермесе.
Сондай-ақ, дәрігерге көрініңіз, егер зақымдану бөліктерінің бетінде сұйықтық, ірің немесе қабық пайда болса, немесе бұл тұстар қызарып, ауырсынатын болса.
Scabies is found among people of all groups and ages around the world.
· Scabies spread by skin-to-skin contact with another person who has scabies.
· Scabies is easily spread among people who are in close contact. Whole families are often affected.
Outbreaks of scabies are more common in nursing homes, nursing facilities, college dorms, and child care centers.
The mites that cause scabies burrow into the skin and lay their eggs. This forms a burrow that looks like a pencil mark. Eggs hatch in 21 days. The itchy rash is an allergic response to the mite.
Pets and animals usually do not spread human scabies. It is also not very likely for scabies to be spread through swimming pools.
A type of scabies called crusted (Norwegian) scabies is a severe infestation with very large numbers of mites. People whose immune systems are weakened are most affected.
· Before treatment, wash clothes and underwear, towels, bedding and sleepwear in hot water and dry at 140°F (60°C) or higher. Dry cleaning also works. If washing or dry cleaning can't be done, keep these items away from the body for at least 72 hours. Away from the body, the mites will die.
· Vacuum carpets and upholstered furniture.
· Use calamine lotion and soak in a cool bath to ease itching.
· Take an oral antihistamine if your provider recommends it for very bad itching.
MEDICINES FROM YOUR HEALTH CARE PROVIDER
The whole family or sexual partners of infected people should be treated, even if they do not have symptoms.
Creams prescribed by your provider are needed to treat scabies.
· The cream most often used is permethrin 5%.
· Other creams include benzyl benzoate, sulfur in petrolatum, and crotamiton.
Apply the medicine all over your body. Creams may be used as a one-time treatment or they may be repeated in 1 week.
For hard to treat cases, the provider may also prescribe a pill known as ivermectin as a one-time dose.
Itching may continue for 2 weeks or more after treatment begins. It will disappear if you follow the provider's treatment plan.
Most cases of scabies can be cured without any long-term problems. A severe case with a lot of scaling or crusting may be a sign that the person has a weakened immune system.
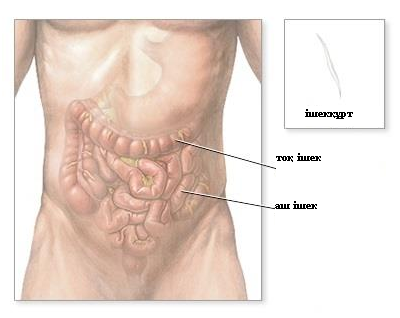
Pinworms are small worms that infect the intestines.
CAUSES
Pinworms are most common in school-age children.
Pinworm eggs are spread directly from person to person. They can also be spread by touching bedding, food, or other items contaminated with the eggs.
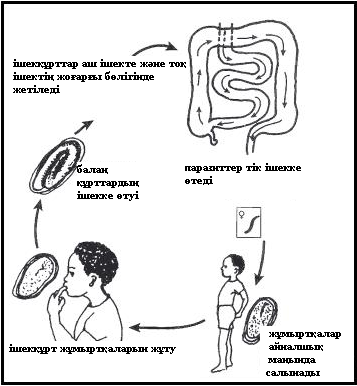
Typically, children are infected by unknowingly touching pinworm eggs and putting their fingers in their mouths. The eggs are swallowed, and eventually hatch in the small intestine. The worms mature in the colon.
Female worms then move to the child's anal area, especially at night, and deposit more eggs. This may cause intense itching. The area may even become infected. When the child scratches the itching anal area, the eggs can get under the child's fingernails. These eggs can be transferred to other children, family members, and items in the house.
SYMPTOMS
Difficulty sleeping due to the itching that occurs during the night
Irritated or infected skin around the anus, from constant scratching
Irritation or discomfort of the vagina in young girls (if an adult worm enters the vagina rather than the anus)
Loss of appetite and weight (uncommon, but can occur in severe infections)
EXAMS AND TESTS
Pinworms can be spotted in the anal area, especially at night when the worms lay their eggs there.
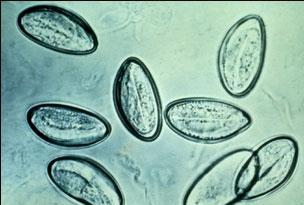
Your doctor or nurse may have you do a tape test. A piece of cellophane tape is pressed against the skin around the anus, and removed. This should be done in the morning before bathing or using the toilet, because bathing and wiping may remove eggs. The doctor will stick the tape to a slide and look for eggs using a microscope.
TREATMENT
Anthelmintic (anti-worm) medicines are used to kill the pinworms (not their eggs). More than one household member is likely to be infected, so the entire household is often treated.
To control the eggs:
Clean toilet seats daily
Keep fingernails short and clean
Wash all bed linens twice a week
Wash hands before meals and after using the toilet
Avoid scratching the infected area around the anus. This can contaminate your fingers and everything else that you touch.
Keep your hands and fingers away from your nose and mouth unless they are freshly washed. Be extra careful while family members are being treated for pinworms.
PROGNOSIS
Pinworm infection is fully treatable.
WHEN TO CONTACT A DOCTOR
Call for an appointment with your doctor if:
You or your child has symptoms of pinworm infection
You have seen pinworms on your child
PREVENTION
Wash hands after using the bathroom and before preparing food. Wash bedding and underclothing frequently, especially those of any affected family members.
· Reactions to medicines and substances such as antibiotics (penicillin, sulfonamides), gold, griseofulvin, isoniazid, opiates, phenothiazines, or vitamin A
For itching that does not go away or is severe, see your health care provider.
In the meantime, you can take steps to help deal with the itch:
· Do not scratch or rub the itchy areas. Keep fingernails short to avoid damaging the skin from scratching. Family members or friends may be able to help by calling attention to your scratching.
· Wear cool, light, loose bedclothes. Avoid wearing rough clothing, such as wool, over an itchy area.
· Take lukewarm baths using little soap and rinse thoroughly. Try a skin-soothing oatmeal or cornstarch bath.
· Apply a soothing lotion after bathing to soften and cool the skin.
· Use moisturizer on the skin, especially in the dry winter months. Dry skin is a common cause of itching.
· Apply cold compresses to an itchy area.
· Avoid prolonged exposure to excessive heat and humidity.
· Do activities that distract you from the itching during the day and make you tired enough to sleep at night.
· Try over-the-counter oral antihistamines such as diphenhydramine (Benadryl). Be aware of possible side effects such as drowsiness.
· Try over-the-counter hydrocortisone cream on itchy areas.
Also call if you have other, unexplained symptoms.
With most itching, you do not need to see a provider. Look for an obvious cause of itching at home.
It is sometimes easy for a parent to find the cause of a child's itching. Looking closely at the skin will help you identify any bites, stings, rashes, dry skin, or irritation.
Have the itching checked out as soon as possible if it keeps returning and does not have a clear cause, you have itching all over your body, or you have hives that keep returning. Unexplained itching may be a symptom of a disease that could be serious.
Your provider will examine you. You'll also be asked about the itching. Questions may include when it began, how long it has lasted, and whether you have it all the time or only at certain times. You may also be asked about medicines you take, whether you have allergies, or if you have been ill recently.
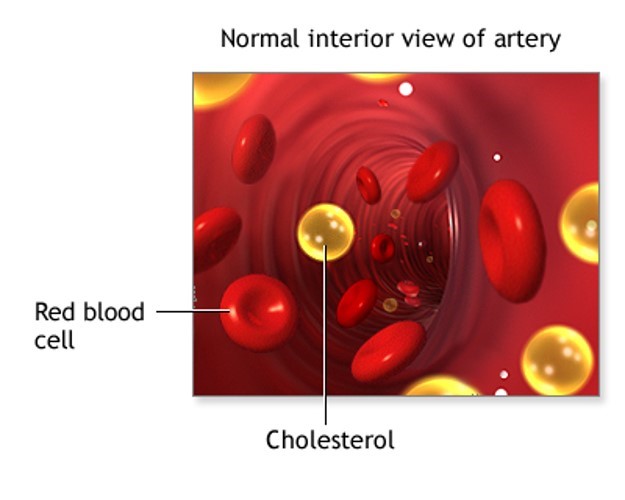
Cholesterol is a soft, wax-like substance found in all parts of the body. Your body needs a little bit of cholesterol to work properly. But too much cholesterol can clog your arteries and lead to heart disease.
Cholesterol blood tests are done to help you and your health care provider better understand your risk for heart disease, stroke, and other problems caused by narrowed or blocked arteries.
The ideal values for all cholesterol results depend on whether you have heart disease, diabetes, or other risk factors. Your provider can tell you what your goal should be.
Some cholesterol is considered good and some is considered bad. Different blood tests can be done to measure each type of cholesterol.
Your provider may order only a total cholesterol level as the first test. It measures all types of cholesterol in your blood.
You may also have a lipid (or coronary risk) profile, which includes:
· Total cholesterol
· Low density lipoprotein (LDL cholesterol)
· High density lipoprotein (HDL cholesterol)
· Triglycerides (another type of fat in your blood)
· Very low density lipoprotein (VLDL cholesterol)
Lipoproteins are made of fat and protein. They carry cholesterol, triglycerides, and other fats, called lipids, in the blood to various parts of the body.
LDL cholesterol is sometimes called "bad" cholesterol. LDL can clog your arteries.
You want your LDL to be low. Too much LDL is linked to heart disease and stroke.
Your LDL is most often considered to be too high if it is 190 mg/dL or higher.
Levels between 70 and 189 mg/dL are most often considered too high if:
· You have diabetes and are between ages 40 and 75
· You have diabetes and a high risk of heart disease
· You have a medium or high risk of heart disease
Health care providers have traditionally set a target level for your LDL cholesterol if you are being treated with medicines to lower your cholesterol.
· Some newer guidelines now suggest that providers no longer need to target a specific number for your LDL cholesterol. Higher strength medicines are used for the highest risk patients.
· However, some guidelines still recommend using specific targets.
You want your HDL cholesterol to be high. Studies of both men and women have shown that the higher your HDL, the lower your risk of coronary artery disease. This is why HDL is sometimes referred to as "good" cholesterol.
HDL cholesterol levels greater than 40 to 60 mg/dL are desired.
VLDL contains the highest amount of triglycerides. VLDL is considered a type of bad cholesterol, because it helps cholesterol build up on the walls of arteries.
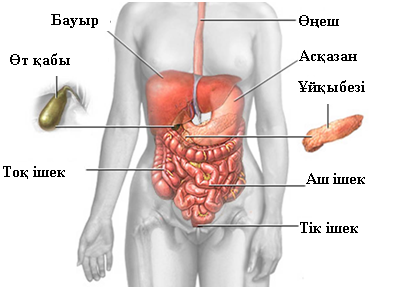
Аноректалдық қатерлі ісік – қатерлі ісіктердің сирек түрі. Айналшық (анус) – ас қорыту жолдарының төменгі ұшындағы саңылау, ол арқылы организмнен нәжіс сыртқа шығарылады. Ол тік ішектің ұшында терінің сыртқы қабатымен қалыптасқан. Аноректалдық қатерлі ісік – айналшықтың тіндерінде қатерлі ісік жасушалары пайда болатын ауру.
Симптомдарына айналшық саңылауы аумағындағы қан кетуі, ауырсыну немесе ісінулердің пайда болуы жатады. Айналшықтың қышуы және бөлінділер де анаоректалдық қатерлі ісіктің симптомдары болуы мүмкін.
Емдеу әдістеріне сәулемен емдеу, химиялық емдеу және хирургиялық араласу жатады. Емдеу әдісі ісіктің таралуына, түріне, өлшеміне және орналасуына байланысты анықталады.