Unconsciousness is when a person is unable to respond to people and activities. Doctors often call this a coma or being in a comatose state.
Other changes in awareness can occur without becoming unconscious. These are called altered mental status or changed mental status. They include sudden confusion, disorientation, or stupor.
Unconsciousness or any other sudden change in mental status must be treated as a medical emergency.
Brief unconsciousness (or fainting) is often a result from dehydration, low blood sugar, or temporary low blood pressure. It can also be caused by serious heart or nervous system problems. A doctor will determine if the affected person needs tests.
Other causes of fainting include straining during a bowel movement (vasovagal syncope), coughing very hard, or breathing very fast (hyperventilating).
If someone is awake but less alert than usual, ask a few simple questions, such as:
· What is your name?
· What is the date?
· How old are you?
· Wrong answers or not being able to answer the question suggest a change in mental status.
If a person is unconscious or has a change in mental status, follow these first aid steps:
1. Call or tell someone to call 911.
2. Check the person's airway, breathing, and pulse frequently. If necessary, begin CPR.
3. If the person is breathing and lying on their back, and you do not think there is a spinal injury, carefully roll the person toward you onto their side. Bend the top leg so both hip and knee are at right angles. Gently tilt their head back to keep the airway open. If breathing or pulse stops at any time, roll the person onto their back and begin CPR.
4. If you think there is a spinal injury, leave the person where you found them (as long as breathing continues). If the person vomits, roll the entire body at one time to their side. Support their neck and back to keep the head and body in the same position while you roll.
5. Keep the person warm until medical help arrives.
6. If you see a person fainting, try to prevent a fall. Lay the person flat on the floor and raise their feet about 12 inches (30 centimeters).
7. If fainting is likely due to low blood sugar, give the person something sweet to eat or drink when they become conscious.
If the person is unconscious from choking:
· Begin CPR. Chest compressions may help dislodge the object.
· If you see something blocking the airway and it is loose, try to remove it. If the object is lodged in the person's throat, do NOT try to grasp it. This can push the object farther into the airway.
· Continue CPR and keep checking to see if the object is dislodged until medical help arrives.
Domestic violence is when a person uses abusive behavior to control a partner or other family member. The abuse can be physical, emotional, economic, or sexual. It can affect people of any age, sex, culture, or class. When domestic violence is aimed at a child, it is called child abuse. Domestic violence is a crime.
Leaving an abusive relationship is not easy. You may be afraid your partner will harm you if you leave, or that you will not have the financial or emotional support you need.
Domestic violence is not your fault. You cannot stop your partner's abuse. But you can find ways to get help for yourself.
· Tell someone. The first step in getting out of an abusive relationship is often telling someone else about it. You can talk to a friend, family member, your health care provider, or a clergy member.
· Have a safety plan. This is a plan in case you need to leave a violent situation right away. Decide where you will go and what you will bring. Gather important items you will need, like credit cards, cash, or papers, in case you need to leave quickly. You can also pack a suitcase and keep it with a family member or friend.
· Get medical care. If you are hurt, get medical care from your provider or at the emergency room.
· Call the police. DO NOT hesitate to call the police if you are in danger. Domestic violence is a crime.
If a friend or family member is being abused, there are many ways you can help.
· Offer support. Your loved one may feel scared, alone, or ashamed. Let him or her know you are there to help however you can.
· DO NOT judge. Leaving an abusive relationship is difficult. Your loved one may stay in the relationship despite the abuse. Or, your loved one may leave and return many times. Try to support these choices, even if you do not agree with them.
· Help with a safety plan. Suggest that your loved one make a safety plan in case of danger. Offer your home as a safe zone if he or she needs to leave, or help find another safe place.
· Find help. Help your loved one connect with a national hotline or a domestic violence agency in your area.
Tooth loss is a process in which one or more teeth come loose and fall out. Tooth loss is normal for deciduous teeth (baby teeth), when they are replaced by a person's adult teeth. Otherwise, losing teeth is undesirable and is the result of injury or disease, such as dental avulsion, tooth decay, and gum disease. The condition of being toothless or missing one or more teeth is called edentulism.
Tooth loss typically begins around age six and continues until age twelve. The upper and lower central incisors are shed at age six to seven years. The upper and lower lateral incisors are shed at seven to eight years. The upper canines are shed at ten to twelve years. The lower canines are shed at nine to twelve years. The upper and lower first molars are shed at nine to eleven years. The upper and lower second molars are shed at ten to twelve years.[1]
As a person ages, their permanent teeth have been exposed to normal mechanical forces, such as chewing, and also more abnormal mechanical forces, such as bruxism (grinding) and traumatic injury. Permanent teeth may also be affected by oral disease.[2] There are many ways in which a person may protect his or her permanent teeth from loss.
The main method of preventing tooth loss is prevention of oral diseases. Tooth loss can be due to tooth decay and gum disease. Tooth decay is caused by increased plaque retention. Bacteria can then invade the plaque and cause dental caries (cavities). If cavities persist untreated for an extended period of time, tooth breakdown occurs.[3] Plaque retention and bacterial presence also affect the gums and bone and their ability to hold the teeth in place. Disease of the gums, known as periodontitis, leads to detachment of the supporting structures from the teeth and their eventual loss. Tooth loss due to tooth decay and gum disease may be prevented by practicing good oral hygiene, and regular check-ups at a dentist's office. Good oral hygiene consists of brushing two times a day with a fluoridated toothpaste and flossing. Dental check-ups should occur every six months. Children or adults who are incapable of caring for their own teeth should be assisted with oral hygiene in order to prevent tooth loss.[4]
In contact sports, risk of mouth trauma and tooth injury is reduced by wearing mouthguards and helmets with a facemask (e.g., a football helmet, a goalie mask).
Nightguards may also be implemented in the case of teeth grinding (bruxism) during sleep. These guards function in limiting the wear and force applied to the teeth. In turn, this minimizes the chance of loss.
In countries such as the United States, Japan, Germany, and Italy, there is a strong relationship between cigarette smoking and tooth loss. Studies have shown that an increase in exposure to cigarette smoking can increase the risk of tooth loss. In addition, studies have also found that when people stop smoking, there is a decrease in tooth loss.[5]
Proper nutrition has been shown to prevent tooth loss by providing the nutrients necessary to maintain enamel strength.[6]
Tooth loss occurs more often in people from the lower end of the socioeconomic scale.[7]
Tooth loss can occur secondary or concomitantly to many diseases. Diseases may cause periodontal disease or bone loss to prompt tooth loss. Consequently, periodontal disease may cause increased infection, which may predispose a person to other diseases. Diseases commonly related to tooth loss include, but are not limited to: cardiovascular disease,[8] cancer,[9] osteoporosis[10] and diabetes mellitus.[11] Therefore, it is important to not only maintain good oral hygiene, but also overall good health.
Maximum preservation and protection of natural teeth is best for eating and chewing; however, there are three basic ways to replace a missing tooth or teeth, including a fixed dental bridge, dentures, and dental implants. Each alternative has its own benefits and drawbacks. It is important to consider a patient's medical, financial, and emotional situation. It is recommended that a patient experiencing tooth loss visits a dentist to discuss which replacement method is best suited for his or her situation. It has been shown that a non-removable replacement, such as a bridge or implant appears to provide patients with the best sense of security and well-being.[12]
2. Jump up^ Baelum V, Luan W-M, Chen X, Fejerskov O (1997). "Predictors of tooth loss over 10 years in adult and elderly Chinese". Community Dent Oral Epidemiol. 25.
4. Jump up^ Li; et al. (2011). "Age, period and cohort analysis of regular dental care behavior and edentulism: a marginal approach.". BMC Oral Health. 11 (9).
5. Jump up^ Hanioka, T., Ojima, M., Tanaka, K., Matsuo, K., Sato, F., and Tanaka H. (2011). "Causal assessment of smoking and tooth loss:a systematic review of observational studies". BMC Public Health. 11: 221. doi:10.1186/1471-2458-11-221.
6. Jump up^ Ioannidou, E; et al. (Nov 11, 2013). "Tooth Loss Strongly Associates with Malnutrition in Chronic Kidney Disease". J Periodontol. 85 (7): 899–907. doi:10.1902/jop.2013.130347. PMID24215204.
Most of the time, your nails are pink and healthy, but sometimes nails have problems. Some of the most common include:
· ingrown nail — when the nail curves down and into the skin, causing pain and, sometimes, an infection
· nail injury — when you drop something on your big toe or catch your finger in a drawer. A bruise may appear under the nail and sometimes the nail falls off. A new one grows in its place.
· nail deformity — when the nail isn't smooth, like a healthy nail. People who bite or pick at their nails a lot can have this problem, but it also can happen if someone has an illness that affects the nail.
· hangnail — when a loose strip of dead skin hangs from the edge of a fingernail. Hangnails hurt if you pull them off.
Some of these problems, such as a minor nail injury or hangnail, can be handled at home by your mom or dad. But infections and more serious nail injuries need a doctor's care. Signs of a nail infection include pain, redness, puffiness (swelling), and maybe some pus.
What Your Nails Have to Say
Don't be surprised if your doctor takes a look at your nails at your next checkup, even if you're having no problems with them. Fingernails provide good clues to a person's overall health.
For instance, when the doctor presses your nails, he or she is checking your blood circulation. By looking at your nails, a doctor may find changes that may be associated with skin problems, lung disease, anemia, and other medical conditions. Your nails are in the know!
Stop any bleeding before applying a dressing to the wound. Apply pressure to the area using a clean and dry absorbent material – such as a bandage, towel or handkerchief – for several minutes.
If the cut is to your hand or arm, raise it above your head to help reduce the flow of blood.
If the injury is to a lower limb, lie down and raise the affected area above the level of your heart.
Clean the wound and apply a dressing
When the wound has stopped bleeding, clean it and cover it with a dressing to help stop it becoming infected.
To do this:
wash and dry your hands thoroughly
clean the wound under drinking-quality running tap water – avoid using antiseptic as it may damage the skin and slow healing
Call Emergency or visit your local walk-in centre, minor injuries unit or GP surgery if there's a risk your wound could become infected, or you think it's already infected.
A wound is at risk of infection if:
it has been contaminated with dirt, pus or other bodily fluids
there was something in the wound before it was cleaned, such as gravel or a shard of glass
you're bleeding from an artery – blood from an artery comes out in spurts with each beat of the heart, and is bright red and usually hard to control
you experience persisting or significant loss of sensation near the wound or you're having trouble moving any body parts
you have received a severe cut to the face – you may require urgent treatment to prevent scarring
you have received a cut to the palm of your hand and it looks infected – these types of infection can spread quickly
there's a possibility a foreign body is still inside the wound
the wound is very large or the injury has caused a lot of tissue damage
In A&E, your wound will be examined to determine whether there's any risk of infection. You may need a booster injection to prevent tetanus, and your wound may be closed with stitches, strips or special glue before a dressing is applied.
If your wound is at risk of infection, it won't usually be closed because this may trap any infection inside. Instead, it will be packed with a non-sticky dressing before being covered with a protective dressing until it's safe to close.
If more pressure is put on a bone than it can stand, it will split or break. A break of any size is called a fracture. If the broken bone punctures the skin, it is called an open fracture (compound fracture).
A stress fracture is a hairline crack in the bone that develops because of repeated or prolonged forces against the bone.
1. Check the person's airway and breathing. If necessary, call 911 and begin rescue breathing, CPR, or bleeding control.
2. Keep the person still and calm.
3. Examine the person closely for other injuries.
4. In most cases, if medical help responds quickly, allow the medical personnel to take further action.
5. If the skin is broken, it should be treated immediately to prevent infection. Call emergency help right away. DO NOT breathe on the wound or probe it. If possible, lightly rinse the wound to remove visible dirt or other contamination, but do not vigorously scrub or flush the wound. Cover with sterile dressings.
6. If needed, immobilize the broken bone with a splint or sling. Possible splints include a rolled up newspaper or strips of wood. Immobilize the area both above and below the injured bone.
7. Apply ice packs to reduce pain and swelling.
8. Take steps to prevent shock. Lay the person flat, elevate the feet about 12 inches (30 centimeters) above the head, and cover the person with a coat or blanket. However, DO NOT move the person if a head, neck, or back injury is suspected.
CHECK BLOOD CIRCULATION
Check the person's blood circulation. Press firmly over the skin beyond the fracture site. (For example, if the fracture is in the leg, press on the foot). It should first blanch white and then "pink up" in about two seconds. Signs that circulation is inadequate include pale or blue skin, numbness or tingling, and loss of pulse.
If circulation is poor and trained personnel are NOT quickly available, try to realign the limb into a normal resting position. This will reduce swelling, pain, and damage to the tissues from lack of blood.
TREAT BLEEDING
Place a dry, clean cloth over the wound to dress it.
If the bleeding continues, apply direct pressure to the site of bleeding. DO NOT apply a tourniquet to the extremity to stop the bleeding unless it is life-threatening.
· DO NOT move the person unless the broken bone is stable.
· DO NOT move a person with an injured hip, pelvis, or upper leg unless it is absolutely necessary. If you must move the person, pull the person to safety by his clothes (such as by the shoulders of a shirt, a belt, or pant-legs).
· DO NOT move a person who has a possible spine injury.
· DO NOT attempt to straighten a bone or change its position unless blood circulation appears hampered.
· DO NOT try to reposition a suspected spine injury.
· The person is not responding or is losing consciousness.
· There is a suspected broken bone in the head, neck, or back.
· There is a suspected broken bone in the hip, pelvis, or upper leg.
· You cannot completely immobilize the injury at the scene by yourself.
· There is severe bleeding.
· An area below the injured joint is pale, cold, clammy, or blue.
· There is a bone projecting through the skin.
Even though other broken bones may not be medical emergencies, they still deserve medical attention. Call your health care provider to find out where and when to be seen.
If a young child refuses to put weight on an arm or leg after an accident, won't move the arm or leg, or you can clearly see a deformity, assume the child has a broken bone and get medical help.
Take the following steps to reduce your risk of a broken bone:
· Wear protective gear while skiing, biking, roller blading, and participating in contact sports. This includes using a helmet, elbow pads, knee pads, and shin pads.
· Create a safe home for young children. Place a gate at stairways and keep windows closed.
· Teach children how to be safe and look out for themselves.
· Supervise children carefully. There is no substitute for supervision, no matter how safe the environment or situation appears to be.
· Prevent falls by not standing on chairs, counter tops, or other unstable objects. Remove throw rugs and electrical cords from floor surfaces. Use handrails on staircases and non-skid mats in bathtubs. These steps are especially important for the elderly.
Your kneecap (patella) sits over the front of your knee joint. As you bend or straighten your knee, the underside of the patella glides over the bones that make up the knee.
Strong tendons help attach the kneecap to the bones and muscles that surround the knee. These tendons are called:
· The patellar tendon (where the kneecap attaches to the shin bone)
· The quadriceps tendon (where the thigh muscles attach to the top of the kneecap)
Anterior knee pain begins when the kneecap does not move properly and rubs against the lower part of the thigh bone. This may occur because:
· The kneecap is in an abnormal position (also called poor alignment of the patellofemoral joint).
· There is tightness or weakness of the muscles on the front and back of your thigh.
· You are doing too much activity that places extra stress on the kneecap (such as running, jumping or twisting, skiing, or playing soccer).
· You have flat feet.
Anterior knee pain is more common in:
· People who are overweight
· People who have had a dislocation, fracture, or other injury to the kneecap
· Runners, jumpers, skiers, bicyclists, and soccer players who exercise often
· Teenagers and healthy young adults, more often girls
Other possible causes of anterior knee pain include:
· Arthritis
· Pinching of the inner lining of the knee during movement (called synovial impingement or plica syndrome)
The health care provider will perform a physical exam. The knee may be tender and mildly swollen. Also, the kneecap may not be perfectly lined up with the thigh bone (femur).
When you flex your knee, you may feel a grinding feeling below the kneecap. Pressing the kneecap when the knee is straightening out may be painful.
Your provider may want you to do a single leg squat to look at muscle imbalance and your core stability.
X-rays are very often normal. However, a special x-ray view of the kneecap may show signs of arthritis or tilting.
Resting the knee for a short period of time and taking nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, naproxen, or aspirin may help relieve pain.
Other things you can do to relieve anterior knee pain include:
· Change the way you exercise.
· Learn exercises to both strengthen and stretch the quadriceps and hamstring muscles.
· Learn exercises to strengthen your core.
· Lose weight (if you are overweight).
· Use special shoe inserts and support devices (orthotics) if you have flat feet.
· Tape your knee to realign the kneecap.
· Wear the correct running or sports shoes.
Rarely, surgery for pain behind the kneecap is needed. During the surgery:
· Kneecap cartilage that has been damaged may be removed.
· Changes may be made to the tendons to help the kneecap move more evenly.
The meniscus is a C-shaped piece of tough, rubbery cartilage that acts as a shock absorber between your shinbone and thighbone. It can be torn if you suddenly twist your knee while bearing weight on it.
A torn meniscus is one of the most common knee injuries. Any activity that causes you to forcefully twist or rotate your knee, especially when putting your full weight on it, can lead to a torn meniscus.
Each of your knees has two menisci — C-shaped pieces of cartilage that act like a cushion between your shinbone and your thighbone. A torn meniscus causes pain, swelling and stiffness. You also might feel a block to knee motion and have trouble extending your knee fully.
Conservative treatment — such as rest, ice and medication — is sometimes enough to relieve the pain of a torn meniscus and give the injury time to heal on its own. In other cases, however, a torn meniscus requires surgical repair.
A torn meniscus can result from any activity that causes you to forcefully twist or rotate your knee, such as aggressive pivoting or sudden stops and turns. Even kneeling, deep squatting or lifting something heavy can sometimes lead to a torn meniscus. In older adults, degenerative changes of the knee can contribute to a torn meniscus with little or no trauma.
Performing activities that involve aggressive twisting and pivoting of the knee puts you at risk of a torn meniscus. The risk is particularly high for athletes — especially those who participate in contact sports, such as football, or activities that involve pivoting, such as tennis or basketball. The risk of a torn meniscus also increases as you get older, due to wear and tear on your knees.
A torn meniscus can lead to knee instability, inability to move your knee normally or persistent knee pain. You might be more likely to develop osteoarthritis in the injured knee.
A torn meniscus often can be identified during a physical exam. Your doctor might move your knee and leg into different positions, watch you walk and ask you to squat to help pinpoint the cause of your signs and symptoms.
Imaging tests
· X-rays. Because a torn meniscus is made of cartilage, it won't show up on X-rays. But X-rays can help rule out other problems with the knee that cause similar symptoms.
· MRI. This uses radio waves and a strong magnetic field to produce detailed images of both hard and soft tissues within your knee. It's the best imaging study to detect a torn meniscus.
Arthroscopy
In some cases, your doctor might use an instrument known as an arthroscope to examine the inside of your knee. The arthroscope is inserted through a tiny incision near your knee.
The device contains a light and a small camera, which transmits an enlarged image of the inside of your knee onto a monitor. If necessary, surgical instruments can be inserted through the arthroscope or through additional small incisions in your knee to trim or repair the tear.
Treatment for a torn meniscus often begins conservatively, depending on the type, size and location of your tear.
Tears associated with arthritis usually improve over time with treatment of the arthritis, so surgery usually isn't indicated. Many other tears that aren't associated with locking or a block to knee motion will become less painful over time, so they also don't require surgery.
Your doctor might recommend:
· Rest. Avoid activities that aggravate your knee pain, especially any activity that causes you to twist, rotate or pivot your knee. If your pain is severe, using crutches can take pressure off your knee and promote healing.
· Ice. Ice can reduce knee pain and swelling. Use a cold pack, a bag of frozen vegetables or a towel filled with ice cubes for about 15 minutes at a time, keeping your knee elevated. Do this every four to six hours the first day or two, and then as often as needed.
· Medication. Over-the-counter pain relievers also can help ease knee pain.
Therapy
Physical therapy can help you strengthen the muscles around your knee and in your legs to help stabilize and support the knee joint.
Surgery
If your knee remains painful despite rehabilitative therapy or if your knee locks, your doctor might recommend surgery. It's sometimes possible to repair a torn meniscus, especially in children and young adults.
If the tear can't be repaired, the meniscus might be surgically trimmed, possibly through tiny incisions using an arthroscope. After surgery, you will need to do exercises to optimize knee strength and stability.
Приапизм деп жыныстық мүшенің ұзақ уақыт бойғы эрекциясын атайды. Жыныстық ынталандырудан немесе қозудан болмаған, қажетті емес, тұрақты эрекция (приапизм) әдетте, ауырсынумен өтеді.
Приапизм – қалыпсыз жағдай, тез арадағы медициналық көмекті қажет етеді. Эрекцияны қолдауға қабілетсіздікке (эректильдік дисфункция) апаратын тіндердің зақымдануын болдырмас үшін уақытылы емдеуді өткізу қажет. Приапизм көбінесе, 5-10 жастағы ұлдар мен 20-50 жастағы ерлерде пайда болады.
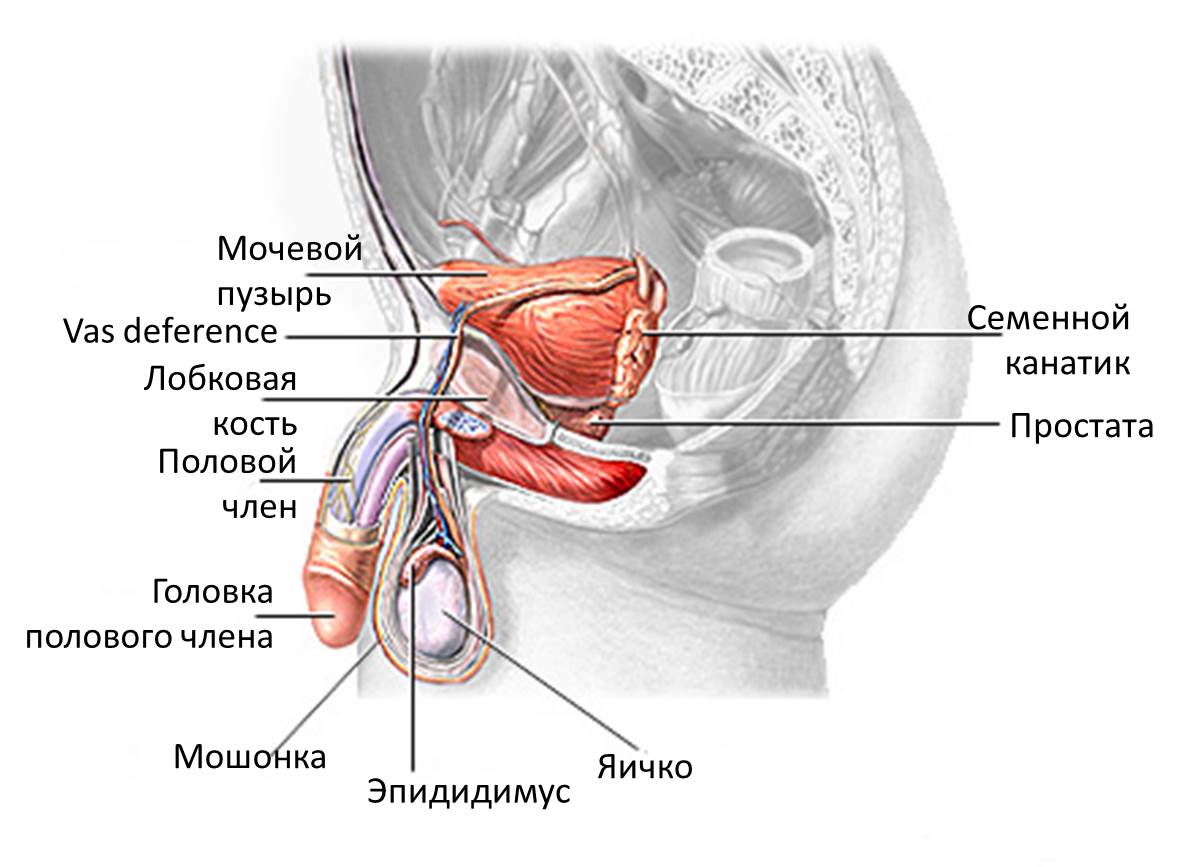
Ерлердің репродуктивтік жүйесі
Приапизм жыныстық ынталандырумен байланысты емес, ауытқулы тұрақты эрекциямен сипатталады. Приапизмнің симптомдары оның түріне қарай ерекшеленеді. Екі негізгі түрі бар: ишемиялық және ишемиялық емесе приапизм.
Егер эрекция төрт сағаттан артыққа созылса, шұғыл медициналық жәрдемге жүгіну қажет. Егер ауырсынатын, ұдайы эрекцияны сезінетін болсаңыз, және ол төрт сағаттан кем уақытта өздігінше өтетін болса, дәрігерге көрініңіз. Бұл көріністердің қайталануын болдырмас үшін, сізге емдеу қажет болуы мүмкін.
Эрекция әдетте, дене немесе психологиялық ынталандыруға жауап ретінде болады. Бұл ынталандыру белгілі бір қантамырларының кеңеюін және босаңсуын туындатады, пенистегі кеуекті тінге қан ағып келуін арттырады. Демек, қан пенисті толтырып, эрекция пайда болады. Ынталандыру аяқталғаннан кейін қан қайтуы орын алады, пенис өзің бос күйіне оралады.
Приапизм осы жүйенің қандай да бір бөлігі – қан, қантамырлары немесе нервтер – қалыпты қан ағымына әсер етіп, оны бұзғанда пайда болады. Кейіннен қажетті емес эрекция сақталады. Приапизмнің пайда болуына ықпал ететін факторлар:
· Қан аурулары, мысалы, лейкемия
· Кейбір дәрілік препараттар, мысалы, антидепрессанттар, антикоагулянттар
· Алкоголь мен есірткі тұтыну
· Жарақаттар
· Басқа факторлар, мысалы, тромб қалыптасуы, жұлынның жарақаты.
Кейбір жағдайда дәрігер приапизмнің себебін анықтай алмайды.
Ишемиялық приапизм күрделі асқынуға апаруы мүмкін. Пенистен қайтпайтын қан оттегіге жұтаң. Эрекция төрт сағаттан артыққа созылса, осы оттегіге жұтаң қан жыныстық мүше тіндерінің зақымдануын және бұзылысын туындатады. Нәтижесінде, емделмеген приапизм келесілерге апаруы мүмкін:
· Эректильдік бұзылысқа – жыныстық мүшенің жыныстық қозу нәтижесінде эрекцияның пайда болуына және қолдауына қабілетсіздігі
· Пенистің деформациясы
Егер сізде немесе балаңызда ауырсынатын эрекция болса, ол төрт сағаттан кем уақытқа созылса, немесе қажетті емес, тұрақты эрекция көріністері болса, дәрігерге көрініңіз. Эрекция төрт сағаттан артық уақытқа созылса, сізге шұғыл медициналық көмек көрсетілуі қажет.
Дәрігер сізге репродуктивтік және несеп-жыныстық ағзалар бойынша маманнан (уролог) кеңес алуды ұсынады.
Егер сізде дәрігер келгенге дейін уақытыңыз болса, оның қоюы мүмкін сұрақтарына жауап дайындаңыз.
· Барлық симптомдарды жазыңыз, сіздің ойыңызша, тұрақты эрекцияға қатысы жоқтарын да.
· Өзіңіз қабылдап жүрген дәрілердің, кез келген дәрумендер мен тағамдық қоспалардың тізімін жасаңыз. Қабылдаған дәрілік препарат немесе тағамдық қоспа туралы дәрігерге хабарлаңыз.
Дәрігерге өзіңіздің қоятын сұрақтарыңызды жазып алуға болады:
· Тұрақты эрекцияның себебі қандай?
· Қандай тексерулер қажет болуы мүмкін?
· Қалай бұл мәселенің болашақта пайда болуының алдын алуға болады?
· Дәрілік препарат қабылдау қажет пе?
· Дене жүктемесінен, жыныстық қатынастан алшақ болу қажет пе? Қаншалықты ұзақ?
· Приапизм эректильдік бұзылыстың даму қаупін арттырады ма?
· Брошюралар немесе қандай сайттарды ұсына аласыз, приапизм туралы толық ақпаратты табу үшін?
Егер сізде басқа сұрақтар пайда болса, немесе бірнәрсені түсінбей қалсаңыз, қарап тексеру кезінде сұрақтарыңызды қойыңыз.
Дәрігер қайталанатын тұрақты эрекция көріністері туралы бірқатар сұрақтар қоюы мүмкін. Бұл келесідей сұрақтар:
· Қашан алғашқыда бұл симптомдар пайда болған?
· Эрекция қаншалықты ұзақ болды?
· Эрекция кезінде ауырсынуды сезіндіңіз бе?
· Оның алдында жыныстық мүшенің немесе шап аумағының жарақаты болды ма?
· Нақты бір заттекті, мысалы, алкоголь, марихуана, кокаин немесе басқа есірткіні тұтынғаннан кейін қажетті емес эрекция болды ма?
· Дәрілік препараттарды қабылдайсыз ба, оның ішінде, эрекциялық бұзылысты емдеу үшін? Қандай да бір шөптесін немесе тағамдық қоспаларды қабылдайсыз ба?
Сондай-ақ, дәрігер талдауды тағайындайды, приапизмнің қандай да бір аурулармен байланысын тексеру үшін.
Дәрігермен кеңеспестен дәрілік препараттарды қабылдауды тоқтатпаңыз. Тұрақты эрекцияны туындатуға қабілетті препараттарды қабылдамаңыз.
Егер эрекция төрт сағаттан артық уақытқа созылса, шұғыл көмек қажет. Алдымен дәрігер приапизмнің түрін анықтайды (ишемиялық немесе ишемиялық емес). Бұл қажет, себебі, емдеуде айырмашылығы бар, сондай-ақ, ишемиялық түрі болуында шұғыл көмек көрсетілуі тиіс.
Приапизмнің түрін анықтау үшін дәрігер бірқатар сұрақтар қояды. Жыныстық мүше, іш, шап аумақатарын қарайды. Дәрігер жыныстық мүшенің сіресуі мен сезімталдығын негізей отырып, приапизмнің түрін анықтайды. Қарау барысында приапизмнің пайда болуына ықпал еткен жарақаттың немесе ісіктің белгілері табылуы мүмкін. Жарақаттар кезінде ишемиялық емес приапизмнің пайда болуы ықтимал.
Диагностикалық тексерулер аурудың түрін анықтау үшін қажет. Қосымша тексерулер оның себебін анықтайды. Егер дәрігер приапизмнің түрін анықтап, сенімді болса, барлық тексерулердің нәтижесі алынғанға дейін шұғыл емдеуді бастай береді. Диагностикалық тексерулерге жататындар:
· Қандағы газдарды анықтау. Тексеру барысында жіңішке ине жыныстық мүшеге енгізіледі, қан үлгісін алу үшін. Қан қошқыл түсті болса – оттегінің мөлшері төмен, бұл ишемиялық приапизм. Егер қан ашық-қызыл түсті болса, приапизм – ишемиялық емес. Қандағы газдарды зертханалық анықтау приапизмнің түрін растайды.
· Қан талдауы. Қандағы эритроциттер мен тромбоциттер санын анықтау қажет. Нәтижелер орақ жасуша тәрізді анемия, қанның басқа аурулары немесе қатерлі ісіктің кейбір түрлері туралы куәландыруы мүмкін.
· УДТ (УЗИ). Допплерография жасалуы мүмкін. Бұл тексеруде ішкі ағзалардың бейнесін алу үшін дыбыстық толқындар қолданылады. Тексеру пенистегі қан ағымын зерттеу үшін тағайындалады. УДТ приапизмнің пайда болуының негізгі себебі болуы мүмкін жарақаттарды, ісіктер мен ауытқуларды анықтауға мүмкіндік береді.
· Токсикологиялық зерттеу. Дәрігер бұл тексеруді науқастың қанында немесе несебінде есірткі немесе приапизмнің себебі болуы мүмкін препараттарды анықтау мақсатында тағайындайды.
Ишемиялық приапизм
Ишемиялық приапизм, пенистен қан ағымы қайтуының бұзылысының нәтижесінде пайда болады, бұл шұғыл жағдай, және емдеудің шұғыл басталуын талап етеді. Емдеу әдетте, жыныстық мүшеден қан айдаудан және дәрілік препараттарды қабылдаудан басталады.
· Аспирация. Пенис жергілікті анестетикті қолданғаннан кейін жансызданғанда, одан жіңішке инемен немесе шприцпен қанның артығы алынады. Бұл ем-шараның аясында жыныстық мүшенің көктамыры физиологиялық ерітіндімен шайылуы мүмкін. Мұндай емдеу ауырсынуды басады, оттегіге жұтаң қанның артығын жояды, және эрекцияның тоқтауына ықпал етеді. Бұл ем-шара эрекция аяқталғанға дейін қайталануы мүмкін.
· Дәрілік препараттар. Пенистің кеуекті тініне альфа-адренергиялық симпатомиметиктердің препараттары енгізілуі мүмкін. Бұл препараттар пенисті қамтамасыз ететін қантамырларын тарылтады. Бұл пенистен қан ағымы қайтатын қантамырының кеңеюіне ықпал етеді. Қажет болса, бұл ем-шара бірнеше сағат ішінде қайталануы мүмкін. Бірақ, жанама әсерлері болуы мүмкін, мысалы, бас ауыруы, бас айналуы, және жоғары артериалдық қысым, әсіресе, егер артериалдық гипертония немесе жүрек аурулары болса.
· Хирургиялық емдеу. Егер басқа емдеу әдістері көмектеспесе, хирург қан ағымын басқа бағытқа бұру және жыныстық мүшеде қалыпты қан ағымын қалпына келтіру үшін құрылғы қондыруы мүмкін (шунт).
· Қосымша емдеу. Егер орақ жасуша тәрізді анемия болса, қосымша емдеу тағайындалады, мысалы, оттегімен емдеу, сусыздануды болдырмас үшін көктамыр арқылы сұйықтық енгізу.
Ишемиялық емес приапизм
Ишемиялық емес приапизм көбінесе, емдеусіз өтеді. Жыныстық мүше тіндерінің зақымдану қаупінің пайда болуы болмайтындықтан, дәрігер бұл жағдайды бақылауға алуды ұсынады. Пенис пен анус аралығындағы аумаққа мұз басу және қысым жасау – эрекцияны басуға көмектесуі мүмкін.
Кейбір жағдайларда пениске қан ағымы келуін тежеу үшін кейіннен еріп кететін арнайы материалдан жасалған затты хирургиялық жолмен қондыру қажет болуы мүмкін. Сондай-ақ, операция жарақаттан кейін қантамырларды және тіндерді қалпына келтіру үшін қажет болуы мүмкін.
Приапизмнің себебіне байланысты бұл жағдайдың қайтадан пайда болуының алдын алу үшін ұсыныстар беріледі:
· Приапизмді туындатқан ауруды емдеу
· Бұл жағдайдың себебі болған дәрілік препараттарды алмастыру
· Алкоголь және есірткі секілді туындатушы факторлардың әсерінің алдын алу
· Фенилэфрин инъекцияларын өздігінше жасау, олар ұзақ уақыт бойғы эрекцияны тоқтатуға көмектеседі
· Гормондарды тежейтін дәрілік препараттар – тек ересек жастағылар үшін.
Пейрони ауруы – бұл жыныстық мүшенің қисаюымен сипатталатын ауру. Кейбір ерлерде Пейрони ауруы жеңіл және симптомдарсыз өтеді. Ал басқаларда эрекция кезінде ауырсынудың пайда болуымен немесе эрекцияның бұзылысымен көрініс береді.
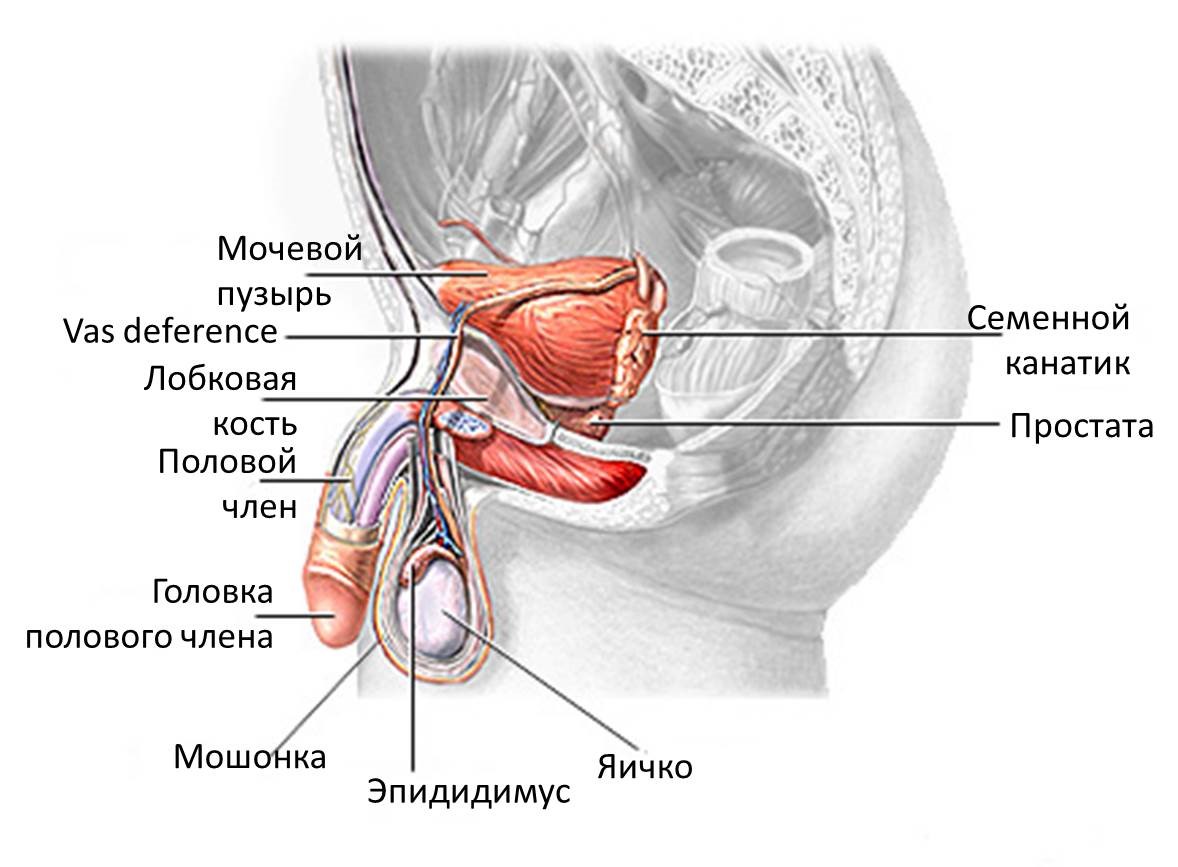
Ерлердің репродуктивтік жүйесіне жыныстық мүше, ұма, ұрықтық түтіктер және қуық асты безі жатады.
Жыныстық мүшенің қисаюы пенистің терісінің астында тыртықты тіннің қалыптасуының салдарынан пайда болады. Тыртықты тіннің пайда болу себебі зерттелмеген. Кейбір ерлерде ол жыныстық мүшенің жарақатынан кейін ұлғая бастайды. Тыртықты тін терінің астынан жоталанып немесе шағын төмпешіктер қатары түрінде шығып тұрады. Алғашқы бірнеше жылдың барысында ол қарқынды ұлғайып, жыныстық мүшенің қисаюының күшеюіне ықпал етеді. Қисаю эрекция кезінде аса айқын байқалады. Бірнеше жылдан кейін тыртықты тіннің өсуі тоқтайды, бірақ, жойылмайды.
Пейрони ауруы толығымен жазылмайды. Кейбір ерлерге калий аминобензоаты немесе Е дәрумені секілді дәрілік препараттар көмектеседі. Калий аминобензоатын емдеуші дәрігер тағайындайды, ал Е дәруменін дәріханадан рецептісіз сатып алуға болады. Е дәруменін дәрігердің тағайындаған мөлшерінен артық қабылдамаңыз. Е дәруменінің үлкен мөлшері ауруды жазуға көмектеспейді. Сонымен қатар, калий аминобензоатын немесе Е дәруменін үлкен мөлшерде қабылдау бауырға зиянын тигізуі мүмкін. Калий аминобензоатын қабылдауда жүрек айнуы және тәбетті жоғалту пайда болуы мүмкін.
Емдеудің басқа нұсқасы – зақымдану ошағына дәрілік препараттың инъекциясын салу. Дәрігер препаратты тікелей тыртықты тінге енгізеді. Әдетте, дәрігер «верапамил» дәрілік препаратын енгізеді. «Верапамил» тыртықты тіннің бұзылуына ықпал етеді, сондай-ақ, зақымданудың жаңа ошақтарының пайда болуының алдын алады. Емдеу курсы, шамамен, 3 айға созылады.
Хирургиялық емдеу эректильдік қабілеті төмендеген және эрекция кезінде ауырсыну пайда болатын ерлерге ұсынылады. Бірнеше хирургиялық әдістеме бар. Емдеудің бір нұсқасы – жыныстық мүшені түзетуге арналған арнайы протезді қондыру. Ол сондай-ақ, ұзақ уақыт бойғы эрекцияны сақтауға көмектеседі. Басқа нұсқа – тыртықты тінді алып тастау. Дәрігер науқасқа хирургиялық емдеудің барлық мүмкін нұсқалары туралы түсіндіріп, қайсысы жарамды екендігін шешуге көмектеседі.