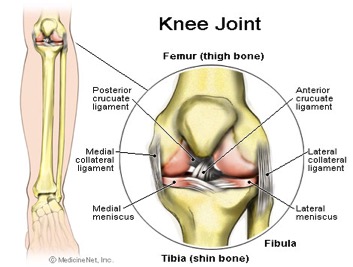
The knee is a joint which has three parts. The thigh bone (femur) meets the large shin bone (tibia) forming the main knee joint. This joint has an inner (medial) and an outer (lateral) compartment. The kneecap (patella) joins the femur to form a third joint, called the patellofemoral joint.
The knee joint is surrounded by a joint capsule with ligaments strapping the inside and outside of the joint (collateral ligaments) as well as crossing within the joint (cruciate ligaments). These ligaments provide stability and strength to the knee joint.
The meniscus is a thickened cartilage pad between the two joints formed by the femur and tibia. The meniscus acts as a smooth surface for the joint to move on. The knee joint is surrounded by fluid-filled sacs called bursae, which serve as gliding surfaces that reduce friction of the tendons. There is a large tendon (patellar tendon) which envelopes the knee cap and attaches to the front of the tibia bone. There are large blood vessels passing through the area behind the knee (referred to as the popliteal space). The large muscles of the thigh move the knee. In the front of the thigh, the quadriceps muscles extend, or straighten, the knee joint by pulling on the patellar tendon. In the back of the thigh, the hamstring muscles flex, or bend, the knee. The knee also rotates slightly under guidance of specific muscles of the thigh.
The knee functions to allow movement of the leg and is critical to normal walking. The knee flexes normally to a maximum of 135 degrees and extends to 0 degrees. The bursae, or fluid-filled sacs, serve as gliding surfaces for the tendons to reduce the force of friction as these tendons move. The knee is a weight-bearing joint. Each meniscus serves to evenly load the surface during weight-bearing and also aids in disbursing joint fluid for joint lubrication.
Injury can affect any of the ligaments, bursae, or tendons surrounding the knee joint. Injury can also affect the ligaments, cartilage, menisci (plural for meniscus), and bones forming the joint. The complexity of the design of the knee joint and the fact that it is an active weight-bearing joint are factors in making the knee one of the most commonly injured joints.
Trauma can cause injury to the ligaments on the inner portion of the knee (medial collateral ligament), the outer portion of the knee (lateral collateral ligament), or within the knee (cruciate ligaments). Injuries to these areas are noticed as immediate pain, but are sometimes difficult to localize. Usually, a collateral ligament injury is felt on the inner or outer portions of the knee. A collateral ligament injury is often associated with local tenderness over the area of the ligament involved. A cruciate ligament injury is felt deep within the knee. It is sometimes noticed with a "popping" sensation with the initial trauma. A ligament injury to the knee is usually painful at rest and may be swollen and warm. The pain is usually worsened by bending the knee, putting weight on the knee, or walking. The severity of the injury can vary from mild (minor stretching or tearing of the ligament fibers, such as a low grade sprain) to severe (complete tear of the ligament fibers). Patients can have more than one area injured in a single traumatic event.
Ligament injuries are initially treated with ice packs and immobilization, with rest and elevation. At first, it is generally recommended to avoid bearing weight on the injured joint and crutches may be required for walking. Some patients are placed in splints or braces to immobilize the joint to decrease pain and promote healing. Arthroscopic or open surgery may be necessary to repair severe injuries.
Surgical repair of ligaments can involve suturing, grafting, and synthetic graft repair. These procedures can be done by either open knee surgery or arthroscopic surgery (described in the section below). The decision to perform various types of surgery depends on the level of damage to the ligaments and the activity expectations of the patient. Many repairs can now be done arthroscopically. However, certain severe injuries will require an open surgical repair. Reconstruction procedures for cruciate ligaments are increasingly successful with current surgical techniques.
The meniscus can be torn with the shearing forces of rotation that are applied to the knee during sharp, rapid motions. This is especially common in sports requiring reaction body movements. There is a higher incidence with aging and degeneration of the underlying cartilage. More than one tear can be present in an individual meniscus. The patient with a meniscal tear may have a rapid onset of a popping sensation with a certain activity or movement of the knee. Occasionally, it is associated with swelling and warmth in the knee. It is often associated with locking or and unstable sensation in the knee joint. The doctor can perform certain maneuvers while examining the knee which might provide further clues to the presence of a meniscal tear.
Routine X-rays, while they do not reveal a meniscal tear, can be used to exclude other problems of the knee joint. The meniscal tear can be diagnosed in one of three ways: arthroscopy , arthrography, or an MRI. Arthroscopy is a surgical technique by which a small diameter video camera is inserted through tiny incisions on the sides of the knee for the purposes of examining and repairing internal knee joint problems. Tiny instruments can be used during arthroscopy to repair the torn meniscus.
Arthrography is a radiology technique whereby a liquid is directly injected into the knee joint and its internal structures thereby become visible on X-ray. An MRI scan is another technique whereby magnetic fields and a computer combine to produce two- or three-dimensional images of the internal structures of the body. It does not use X-rays, and can give accurate information about the internal structures of the knee when considering a surgical intervention. Meniscal tears are often visible using an MRI scanner. MRI scans have largely replaced arthrography in diagnosing meniscal tears of the knee. Meniscal tears are generally repaired arthroscopically.
Tendinitis of the knee occurs in the front of the knee below the kneecap at the patellar tendon (patellar tendinitis) or in the back of the knee at the popliteal tendon (popliteal tendinitis). Tendinitis is an inflammation of the tendon, which is often produced by events, such as jumping, that strain the tendon. Patellar tendinitis, therefore, also has the name "jumper's knee." Tendinitis is diagnosed based on the presence of pain and tenderness localized to the tendon. It is treated with a combination of ice packs, immobilization with a knee brace as needed, rest, and anti-inflammatory medications. Gradually, exercise programs can rehabilitate the tissues in and around the involved tendon. Cortisone injections, which can be given for tendinitis elsewhere, are generally avoided in patellar tendinitis because there are reports of risk of tendon rupture as a result. In severe cases, surgery may be required. A rupture of the tendon below or above the kneecap can occur. When it does, there may be bleeding within the knee joint and extreme pain with any knee movement. Surgical repair of the ruptured tendon is often necessary.
With severe knee trauma, such as motor vehicle accidents and impact traumas, bone breakage (fracture) of any of the three bones of the knee can occur. Bone fractures within the knee joint can be serious and may require surgical repair as well as immobilization with casting or other supports.
Pain can occur in the knee from diseases or conditions that involve the knee joint, the soft tissues and bones surrounding the knee, or the nerves that supply sensation to the knee area. The knee joint is commonly affected by rheumatic diseases, immune diseases that affect various tissues of the body including the joints.
Arthritis is associated with pain and swelling of a joint. The causes of knee joint pain and swelling range from noninflammatory types of arthritis such as osteoarthritis, which is a degeneration of the cartilage of the knee, to inflammatory types of arthritis (such as rheumatoid arthritis or gout). Treatment of the arthritis is directed according to the nature of the specific type of arthritis.
Infections of the bone or joint can rarely be a serious cause of knee pain and have associated signs of infection including fever, extreme heat, warmth of the joint, chills of the body, and may be associated with puncture wounds in the area around the knee.
Tumors involving the joint are extremely rare. They can cause problems with local pain.
The collateral ligament on the inside of the knee joint can become calcified and is referred to as Pellegrini-Stieda syndrome. With this condition, the knee can become inflamed and can be treated conservatively with ice packs, immobilization, and rest. Infrequently, it requires a local injection of corticosteroids.
Chondromalacia refers to a softening of the cartilage under the kneecap (patella). It is a common cause of deep knee pain and stiffness in younger women and can be associated with pain and stiffness after prolonged sitting and climbing stairs or hills. While treatment with anti-inflammatory medications, ice packs, and rest can help, long-term relief is best achieved by strengthening exercises for the muscles of the front of the thigh.
Bursitis of the knee commonly occurs on the inside of the knee (anserine bursitis) and the front of the kneecap (patellar bursitis, or "housemaid's knee"). Bursitis is generally treated with ice packs, immobilization, and anti-inflammatory drugs such as ibuprofen (Advil, Motrin) or aspirin and may require local injections of corticosteroids (cortisone medication) as well as exercise therapy to develop the musculature of the front of the thigh.
The meniscus is a C-shaped piece of tough, rubbery cartilage that acts as a shock absorber between your shinbone and thighbone. It can be torn if you suddenly twist your knee while bearing weight on it.
A torn meniscus is one of the most common knee injuries. Any activity that causes you to forcefully twist or rotate your knee, especially when putting your full weight on it, can lead to a torn meniscus.
Each of your knees has two menisci — C-shaped pieces of cartilage that act like a cushion between your shinbone and your thighbone. A torn meniscus causes pain, swelling and stiffness. You also might feel a block to knee motion and have trouble extending your knee fully.
Conservative treatment — such as rest, ice and medication — is sometimes enough to relieve the pain of a torn meniscus and give the injury time to heal on its own. In other cases, however, a torn meniscus requires surgical repair.
A torn meniscus can result from any activity that causes you to forcefully twist or rotate your knee, such as aggressive pivoting or sudden stops and turns. Even kneeling, deep squatting or lifting something heavy can sometimes lead to a torn meniscus. In older adults, degenerative changes of the knee can contribute to a torn meniscus with little or no trauma.
Performing activities that involve aggressive twisting and pivoting of the knee puts you at risk of a torn meniscus. The risk is particularly high for athletes — especially those who participate in contact sports, such as football, or activities that involve pivoting, such as tennis or basketball. The risk of a torn meniscus also increases as you get older, due to wear and tear on your knees.
A torn meniscus can lead to knee instability, inability to move your knee normally or persistent knee pain. You might be more likely to develop osteoarthritis in the injured knee.
A torn meniscus often can be identified during a physical exam. Your doctor might move your knee and leg into different positions, watch you walk and ask you to squat to help pinpoint the cause of your signs and symptoms.
Imaging tests
· X-rays. Because a torn meniscus is made of cartilage, it won't show up on X-rays. But X-rays can help rule out other problems with the knee that cause similar symptoms.
· MRI. This uses radio waves and a strong magnetic field to produce detailed images of both hard and soft tissues within your knee. It's the best imaging study to detect a torn meniscus.
Arthroscopy
In some cases, your doctor might use an instrument known as an arthroscope to examine the inside of your knee. The arthroscope is inserted through a tiny incision near your knee.
The device contains a light and a small camera, which transmits an enlarged image of the inside of your knee onto a monitor. If necessary, surgical instruments can be inserted through the arthroscope or through additional small incisions in your knee to trim or repair the tear.
Treatment for a torn meniscus often begins conservatively, depending on the type, size and location of your tear.
Tears associated with arthritis usually improve over time with treatment of the arthritis, so surgery usually isn't indicated. Many other tears that aren't associated with locking or a block to knee motion will become less painful over time, so they also don't require surgery.
Your doctor might recommend:
· Rest. Avoid activities that aggravate your knee pain, especially any activity that causes you to twist, rotate or pivot your knee. If your pain is severe, using crutches can take pressure off your knee and promote healing.
· Ice. Ice can reduce knee pain and swelling. Use a cold pack, a bag of frozen vegetables or a towel filled with ice cubes for about 15 minutes at a time, keeping your knee elevated. Do this every four to six hours the first day or two, and then as often as needed.
· Medication. Over-the-counter pain relievers also can help ease knee pain.
Therapy
Physical therapy can help you strengthen the muscles around your knee and in your legs to help stabilize and support the knee joint.
Surgery
If your knee remains painful despite rehabilitative therapy or if your knee locks, your doctor might recommend surgery. It's sometimes possible to repair a torn meniscus, especially in children and young adults.
If the tear can't be repaired, the meniscus might be surgically trimmed, possibly through tiny incisions using an arthroscope. After surgery, you will need to do exercises to optimize knee strength and stability.
Хондрогенез (также называется хондромаляция) – это патологическое размягчение или разрушение гладкого хряща, в основном того, который покрывает заднюю сторону надколенной чашки. Размягченный хрящ может вызывать боль каждый раз, когда на оборотную сторону надколенной чашки оказывается давление при приседании на колени, спуске с лестницы и длительном сидении.
Мениски коленного сустава представляют собой хрящевые прокладки, которые исполняют роль амортизаторов в суставе, а так же стабилизируют коленный сустав. При движениях в коленном суставе мениски сжимаются, их форма изменяется. Это хрящевинной структуры образования, которые участвуют в формировании коленного сустава. Мениски располагаются на мыщелках большеберцовых костей.
Менисков коленного сустава два:
наружный (латеральный) имеет форму буквы О
внутренний (медиальный) имеет форму буквы С.
Спереди сустава они соединяются поперечной связкой. Наружный мениск более подвижен, чем внутренний, поэтому его травматические повреждения происходят реже.
Внутренний мениск менее подвижен и связан с внутренней боковой связкой коленного сустава, что часто вызывает его сочетанное со связкой поражение. Сбоку от сустава мениски сращены с капсулой сустава и имеют кровоснабжение от артерий капсулы. Внутренние части находятся в глубине сустава и собственного кровоснабжения не имеют, а питание их тканей осуществляется за счет циркуляции внутрисуставной жидкости. Поэтому повреждения менисков рядом с капсулой сустава срастаются хорошо, а разрывы внутренней части, в глубине коленного сустава не срастаются совсем.
Возникают повреждения менисков при резких движениях голени с поворотом в коленном суставе, но при фиксированной стопе. Реже разрывы менисков происходят при приседании, при прыжках. Часто травма, которая привела к разрыву мениска, может быть незначительной. Чаще всего травмируется внутренний мениск (до 75 %). При этом зачастую вместе с повреждением внутреннего мениска отмечается разрыв передней крестообразной и внутренней боковой связки. Оторванная часть мениска, связанная с телом мениска может перемещаться в полости сустава и ущемляется между суставными поверхностями бедренной и большеберцовой костей.
Клиника. Если сразу после травмы колена возникает сильная боль, невозможно ни согнуть, ни разогнуть ногу, появляется ощущение щелчка и возможного заклинивания сустава – это сигнал SOS. Пациент жалуется на сильные боли, нарушение движений в коленном суставе. Иногда разрыв мениска сопровождается кровотечением в коленный сустав (гемартроз), но чаще возникает реактивное воспаление внутренней оболочки сустава – синовит. Больной удерживает ногу в согнутом состоянии, потому что боль усиливается при разгибании, особенно если произошла блокада сустава. При прощупывании обнаруживается боль в проекции поврежденного мениска, иногда прощупывается эластичный валик, который перекатывается по наружной поверхности суставной щели при разгибании в суставе. Этот симптом называется симптом щелчка или переката.
Диагностика. Рентген хорош только для диагностики повреждений костей. Мениски он не "видит". Улучшенный его вариант - компьютерная рентгенограмма - тоже. УЗИ информативно только в 50-60% всех возможных повреждений сустава. Ответ на 95% диагностических вопросов может дать только метод магнитно-резонансной томографии (МРТ). Он позволяет увидеть даже те переломы, что остаются незамеченными рентгеном, и точно определить разрыв мениска.
Лечение. Если диагноз "разрыв мениска" поставлен, то оперировать колено надо быстрее, пока не стал разрушаться суставной хрящ. Удалять разорванный мениск или сшивать? Это решает врач. Но предпочтительнее сшивание. Особенно биорассасывающимися нитями. Это потребует потом 3-4 недели обездвижения сустава, но дело того стоит. На удаление мениска хирург идет, только если сохранять уже нечего из-за его давнего нелеченного разрыва.