Ми қан айналымының өтпелі ишемиялық бұзылуы- бұл уақытша мидың аймақтық қан ағымының бұзылысы. Осы жақын арада ұстама болуы мүмкін екендігіне белгі болып табылады.
Артериядағы қан ұйындысы, қан қысымының төмендеуі немесе жүрек соғуының бұзылысы мидың қандануын төмендетеді, ми қан айналымының уақытша ишемиялық бұзылуының салдары болып табылады.
Ми қан айналымының өтпелі ишемиялық бұзылыстарының белгілері ұстаманың белгілеріне ұқсас болып келеді. Оларға:
Көрүдің бұзылыстары.
Қиын сөйлеу немесе ерекше мінез-құлық және ойлау үрдістері.
Есін жоғалту
Талма.
Әлсіздік және дененің бір жағының жансыздануы.
Талмадан айырмашылығы, ми қан айналымының өтпелі ишемиялық бұзылуы ұзақ мерзімді симптомдарды тудырмайды. Әдетте белгілер 10-20 минуттан кейін жоғалады, бірақ олар 24 сағатқа дейін созылуы да мүмкін.
Ми қан айналымының уақытша ишемиясы - бұл қауіп төндіретін талманы ескертеді.
Парвовирустық инфекция кезінде келесі симптомдар байқалады:
Ашық түсті теңбіл бөріткен алдымен беттің ұшында пайда болады (бетті «алау» шалғандай). Одан кейін денеге, қол-аяққа тарайды. Парвовирустық инфекцияда ортадан шетке қарай жойылады, тор-шілтер тәрізденеді. Бөріткен 1-2 апта ішінде толығымен өтеді.
Қызба
Буынның ауырсынуы
Уақытша анемия (қанда функционалдық толыққұнды қызыл жасушалар-эритроциттердің мөлшері төмендейтін жағдай).
Ауруды анықтау үшін дәрігердің қарауы жеткілікті, себебі, парвовирустық инфекцияның тек өзіне ғана тән бөріткені болады. В19 парвовирусына қарсы антиденелерге (қандағы ақуыздық қосылыстар, олар бактериялар мен вирустар секілді бөгде организмдерді анықтап, жоюға мүмкіндік береді) қант талдауы диагнозды нақтылай алады.
Парвовирустық инфекция кезінде арнайы емдеу қажет болмайды. Егер балада қызба болса, жағдайды жақсарту үшін қызуды түсіретін кез келген препарат берілуі мүмкін.
Балаларда ауру жиі жеңіл түрде өтсе де, кейде сирек асқынулар болады, алайда, егер парвовирустық инфекцияға жүкті әйел шалдықса, бұл ұрықтың дамуында күрделі бұзылыстарға апаруы мүмкін.
Note: Serum is the part of blood that doesn't contain cells.
Sodium, potassium, and chloride levels can also be measured as part of a basic metabolic panel. A more complete test, called comprehensive metabolic panel, can test for these several more electrolytes.
The electrolytes - urine test measures electrolytes in urine. It test the levels of calcium, chloride, potassium, sodium, and other electrolytes.
Repetitive motion injuries are among the most common injuries in the United States. All of these disorders are made worse by the repetitive actions of daily living.
Repetitive motion injuries make up over 50% of all athletic-related injuries seen by doctors and result in huge losses in terms of cost to the workforce. Simple everyday actions, such as throwing a ball, scrubbing a floor, or jogging, can lead to this condition.
The most common types of repetitive motion injuries are tendinitis and bursitis. These two disorders are difficult to differentiate and many times may coexist.
Tendinitis
A tendon is a white fibrous tissue that connects muscle to bone and allows for movement at all joints throughout the human body. Because tendons must be able to bear all of the weight of the attached muscle, they are very strong.
Tendinitis is an inflammation of the tendon. (Whenever you see "-itis" at the end of a word, think "inflammation.")
Males are slightly more likely to have this disorder.
The inflammation of the tendon usually occurs at the site of insertion into bone.
Tendons run through a lubricating sheath where they connect into muscle, and this sheath also may become inflamed. This condition is known as tenosynovitis.
Tenosynovitis is almost identical to tendinitis because both have identical causes, symptoms, and treatment.
Tenosynovitis of the wrist may be involved in carpal tunnel syndrome, the most common compression nerve disorder, but this cause-and-effect relationship has never been proven.
Bursitis
A bursa is a small pouch or sac that is found over an area where friction may develop and serves to cushion or lubricate the area between tendon and bone.
Bursitis is inflammation of a bursa sac.
Over 150 bursae are in the body.
Most bursae are present at birth, but some come into existence in sites of repetitive pressure.
Common areas where bursitis can occur include the elbow, knee, and hip.
Different types of bursitis include traumatic, infectious, and gouty.
Traumatic bursitis is the type involved with repetitive motion injuries.
Traumatic bursitis is most common in people younger than 35 years.
Repetitive motion disorders develop because of microscopic tears in the tissue. When the body is unable to repair the tears in the tissue as fast as they are being made, inflammation occurs, leading to the sensation of pain. Causes of repetitive motion injuries include:
Tendinitis: The most common symptom associated with tendinitis is pain over the site involved. Tendinitis is made worse by active motion of the inflamed tendon. The skin overlying the inflamed tendon may be red and warm to the touch.
Biceps: The painful spot is usually in the groove where the arm meets the shoulder. You can reproduce the pain by flexing your elbow at 90 and trying to turn your hand palm up (called supination) against resistance.
Tennis elbow: This pain is in the elbow and is reproduced by cocking your wrist back (extending the wrist) as if you are bringing a tennis racket back to hit the ball.
Golfer's elbow: This pain also occurs in the elbow but is made worse by flexing the wrist forward as if you are hitting a golf ball.
Rotator cuff: Raising your arm out to the side reproduces this pain. The painful area is usually over the affected shoulder.
Bursitis: Common symptoms include pain, tenderness, and decreased range of motion over affected area. Redness, swelling, and a crunchy feeling when the joint is moved (crepitus) may also occur.
Knee: This condition involves swelling over the bottom part of the kneecap that is red and warm to the touch. Usually, the range of motion of the knee will be less because of the pain that bending and straightening the knee causes.
Elbow: Pain, swelling, and redness are found over the elbow. The pain gets worse when you flex and extend your arm at the elbow.
Hip: Your pain is increased by walking or by lying on the affected side. Bringing your leg away from and toward the midline of the body can also reproduce the pain.
When to call the doctor Call your doctor if you have any of the following symptoms:
Pain with movement of arms and legs
Tenderness over a joint or where a tendon connects
Redness and increased warmth over a joint
Pain that wakes you from sleep
Inability to sleep on affected side
Inability to carry on normal activities of daily living (such as brushing your teeth or taking a shower)
When to go to the hospital
Certain signs and symptoms may mean that you have an infection and should be seen by a doctor immediately. Seek immediate medical care for any of the following symptoms:
The diagnosis of tendinitis is most often made based on history and a physical examination.
Imaging studies may help confirm the diagnosis. The imaging study of choice is the MRI. An MRI gives a very detailed picture and can identify a tear, rupture, inflammation, or other disease processes. An MRI is not useful in visualizing inflammation of the tendon sheath, tenosynovitis, unless fluid is present within the sheath itself.
Bursitis
Your doctor will check if your bursitis has an inflammatory or an infectious cause. The elbow and knee have a higher risk of having an infectious cause, so fluid will probably be drained from your joint to be checked for bacterial infection.
Conditions that place you at a higher risk for infectious bursitis include:
Home care for a painful or swollen joint should include elevation and not moving it until your doctor can be contacted. You can also use ice for relief of pain and swelling.
Most authorities recommend icing 2-3 times a day for 20-30 minutes each time.
Wrap ice or a bag of frozen vegetables in a towel and place it on the area.
If your shoulder is involved, you should not keep it immobile for more than 24-48 hours because your shoulder may become frozen and have decreased range of motion.
Tendinitis is best treated with immobilization and ice during the early phase and moist heat during the long-term phase.
Bands placed around the elbow may be used for tennis elbow and golfer's elbow.
Nonsteroidal anti-inflammatory drugs (NSAIDs, such as aspirin, naproxen, or ibuprofen) may be prescribed to reduce the inflammation. All NSAIDs should be taken with food or milk to avoid stomach upset.
If your tendinitis or bursitis is not helped by NSAIDs, the doctor may choose to inject steroids into the surrounding area of inflammation. As a rule, you should not have more than 3 injections into the same area within a 12-month period.
You should begin graduated range-of-motion exercise once your symptoms begin to improve.
An exception to this type of treatment is shoulder involvement.
The shoulder should not be immobilized for more than 24-48 hours in order to minimize frozen shoulder, called adhesive capsulitis.
You should have physical therapy in addition to ultrasound and warm water baths.
The goal in treatment of shoulder tendinitis is first and foremost to maintain full range of motion of the shoulder joint. Relieving the symptoms is secondary.
The treatment of inflammatory bursitis is similar to that of tendinitis.
Use rest and ice, and elevate your arm or leg.
Alternative treatments include pain-killing creams, capsaicin cream (an over-the-counter pain relief cream made from an ingredient of cayenne pepper), and steroid medications if you are able to take them.
If your bursitis is caused by an infection, treatment will include the appropriate antibiotics.
Steroid injection may be used but only for inflammatory bursitis. Steroid injections should be avoided in infectious bursitis because they may increase the body's susceptibility to infection.
The prevention of tendinitis and bursitis is similar in most respects.
Do adequate warm-up and cool-down maneuvers (crucial to proper tendon and bursae health).
Avoid activity that makes your injury flare up. This will speed healing of both tendinitis and bursitis.
If using a hedge clipper caused you pain, avoid this activity and others like it.
If reaching overhead in your work has caused a repetitive motion injury, your occupational health manager may be able to redesign your job so you won't have to reach overhead.
Practice range-of-motion exercises, especially with tendinitis. These are important to ensure minimal decrease in function.
Use splints or bands to decrease the strain on a tendon that occurs with sporting activities, such as tennis and golf. These devices may be bought over-the-counter or obtained from your doctor.
Sickle cell anemia is a disease passed down through families. The red blood cells that are normally shaped like a disc take on a sickle or crescent shape. Red blood cells carry oxygen throughout the body.
Sickle cell anemia is caused by an abnormal type of hemoglobin called hemoglobin S. Hemoglobin is a protein inside red blood cells that carries oxygen.
· Hemoglobin S changes the red blood cells. The red blood cells become fragile and shaped like crescents or sickles.
· The abnormal cells deliver less oxygen to the body's tissues.
· They can also easily get stuck in small blood vessels and break into pieces. This can interrupt healthy blood flow and cut down even more on the amount of oxygen flowing to body tissues.
Sickle cell anemia is inherited from both parents. If you get the sickle cell gene from only 1 parent, you will have sickle cell trait. People with sickle cell trait do not have the symptoms of sickle cell anemia.
Sickle cell disease is much more common in people of African and Mediterranean descent. It is also seen in people from South and Central America, the Caribbean, and the Middle East.
Symptoms usually do not occur until after the age of 4 months.
Almost all people with sickle cell anemia have painful episodes called crises. These can last from hours to days. Crises can cause pain in the lower back, leg, joints, and chest.
Some people have 1 episode every few years. Others have many episodes each year. The crises can be severe enough to require a hospital stay.
When the anemia becomes more severe, symptoms may include:
The goal of treatment is to manage and control symptoms, and to limit the number of crises. People with sickle cell disease need ongoing treatment, even when not having a crisis.
People with this condition should take folic acid supplements. Folic acid helps make new red blood cells.
Treatment for a sickle cell crisis includes:
· Blood transfusions (may also be given regularly to prevent stroke)
· Pain medicines
· Plenty of fluids
Other treatments for sickle cell anemia may include:
· Hydroxyurea (Hydrea), which helps reduce the number of pain episodes (including chest pain and breathing problems) in some people
· Antibiotics, which help prevent bacterial infections that are common in children with sickle cell disease
· Medicines that reduce the amount of iron in the body.
Treatments that may be needed to manage complications of sickle cell anemia include:
· Treatment for overuse or abuse of narcotic pain medicines
· Wound care for leg ulcers
Bone marrow or stem cell transplants can cure sickle cell anemia, but this treatment is not an option for most people. Sickle cell anemia people often cannot find well-matched stem cell donors.
People with sickle cell disease should have the following vaccinations to lower the risk of infection:
In the past, people with sickle cell disease often died between ages 20 and 40. Thanks to a modern care, people now can live to the age of 50 and beyond.
Causes of death include organ failure and infection.
Multiple myeloma is a cancer that forms in a type of white blood cell called a plasma cell. Plasma cells help you fight infections by making antibodies that recognize and attack germs.
Multiple myeloma causes cancer cells to accumulate in the bone marrow, where they crowd out healthy blood cells. Rather than produce helpful antibodies, the cancer cells produce abnormal proteins that can cause kidney problems.
Treatment for multiple myeloma isn't always necessary. If you're not experiencing signs and symptoms, you may not require treatment. If signs and symptoms develop, a number of treatments can help control your multiple myeloma.
Signs and symptoms of multiple myeloma can vary and, early in the disease, there may be none.
When signs and symptoms do occur, they can include:
Make an appointment with your doctor if you have any persistent signs and symptoms that worry you.
It's not clear what causes myeloma.
Doctors know that myeloma begins with one abnormal plasma cell in your bone marrow — the soft, blood-producing tissue that fills in the center of most of your bones. The abnormal cell multiplies rapidly.
Because cancer cells don't mature and then die as normal cells do, they accumulate, eventually overwhelming the production of healthy cells. In the bone marrow, myeloma cells crowd out healthy white blood cells and red blood cells, leading to fatigue and an inability to fight infections.
The myeloma cells continue trying to produce antibodies, as healthy plasma cells do, but the myeloma cells produce abnormal antibodies that the body can't use. Instead, the abnormal antibodies (monoclonal proteins, or M proteins) build up in the body and cause problems, such as damage to the kidneys.
Multiple myeloma almost always starts out as a relatively benign condition called monoclonal gammopathy of undetermined significance (MGUS).
In the United States, about 3 percent of people older than age 50 have MGUS. Each year, about 1 percent of people with MGUS develop multiple myeloma or a related cancer.
MGUS, like multiple myeloma, is marked by the presence of M proteins — produced by abnormal plasma cells — in your blood. However, in MGUS, the levels of M proteins are lower and no damage to the body occurs.
Factors that may increase your risk of multiple myeloma include:
· Increasing age. Your risk of multiple myeloma increases as you age, with most people diagnosed in their mid-60s.
· Male sex. Men are more likely to develop the disease than are women.
· Black race. Blacks are about twice as likely to develop multiple myeloma as are whites.
· History of a monoclonal gammopathy of undetermined significance (MGUS). Every year 1 percent of the people with MGUS in the United States develop multiple myeloma.
Complications of multiple myeloma include:
· Frequent infections. Myeloma cells inhibit your body's ability to fight infections.
· Bone problems. Multiple myeloma also can affect your bones, leading to bone pain, thinning bones and broken bones.
· Reduced kidney function. Multiple myeloma may cause problems with kidney function, including kidney failure. Higher calcium levels in the blood related to eroding bones can interfere with your kidneys' ability to filter your blood's waste. The proteins produced by the myeloma cells can cause similar problems.
· Low red blood cell count (anemia). As myeloma cells crowd out normal blood cells, multiple myeloma can also cause anemia and other blood problems.
If you have any signs or symptoms that worry you, make an appointment with your doctor.
If you're diagnosed with multiple myeloma, you'll likely be referred to a doctor who specializes in treating blood and bone marrow disorders (hematologist) or a doctor who specializes in treating cancer (oncologist).
Because appointments can be brief and because there's often a lot of ground to cover, it's a good idea to be well-prepared. Here's some information to help you get ready and know what to expect from your doctor.
· Note symptoms you're experiencing. If you have had signs and symptoms of illness or are just not feeling well, write down those details before your appointment. Your doctor will also want to know when you first noticed these symptoms and whether they've changed over time.
· List other medical conditions. Your doctor will be especially interested to know if you've been diagnosed with any other plasma disorders, such as monoclonal gammopathy of undetermined significance (MGUS).
· Make a list of your medications. Include any prescription or over-the-counter medications you're taking, as well as all vitamins, supplements and herbal remedies.
· Take a family member or friend along. Sometimes it can be difficult to remember all the information provided during an appointment. Someone who accompanies you may remember something that you missed or forgot.
· Write down questions to ask your doctor.
Questions to ask your doctor at your initial appointment include:
· What may be causing my symptoms or condition?
· Are there any other possible causes?
· What kinds of tests do I need?
· What do you recommend for next steps in determining my diagnosis and treatment?
· Are there any restrictions that I need to follow in the meantime?
Questions to consider if your doctor refers you to a specialist include:
· Do I have multiple myeloma?
· What stage of myeloma do I have?
· Does my myeloma have any high-risk features?
· What are the goals of treatment in my case?
· What treatment do you recommend?
· I have these other health problems. How can I best treat them together with multiple myeloma?
· What are the possible side effects of treatment?
· If the first treatment isn't successful, what will we try next?
· Am I a candidate for stem cell transplantation?
· Do I need a medicine to strengthen my bones?
· What is the outlook for my condition?
In addition to the questions that you've prepared to ask your doctor, don't hesitate to ask questions during your appointment at any time that you don't understand something.
Your doctor is likely to ask you a number of questions. Thinking about your answers ahead of time can help you make the most of your appointment. A doctor who sees you for possible multiple myeloma may ask:
· What are your symptoms, if any?
· When did you first begin experiencing symptoms?
· How have your symptoms changed over time?
· Do your symptoms include bone pain? Where?
· Do your symptoms include nausea, lost appetite or weight loss?
· Do your symptoms include weakness or fatigue?
· Have you had repeated infections, such as pneumonia, sinusitis, bladder or kidney infections, skin infections, or shingles?
· Have you noticed any changes in your bowel habits?
· Have you been more thirsty or urinated more than usual?
· What else concerns you?
· Do you have any family history of plasma disorders such as MGUS?
· Have you been diagnosed or treated for any other medical conditions?
· Do you have a history of blood clots?
· What medications are you taking?
In some cases, your doctor may detect multiple myeloma accidentally when you undergo a blood test for some other condition. In other cases, your doctor may suspect multiple myeloma based on your signs and symptoms.
Tests and procedures used to diagnose multiple myeloma include:
· Blood tests. Laboratory analysis of your blood may reveal the M proteins produced by myeloma cells. Another abnormal protein produced by myeloma cells — called beta-2-microglobulin — may be detected in your blood and give your doctor clues about the aggressiveness of your myeloma.
Additionally, blood tests to examine your kidney function, blood cell counts, calcium levels and uric acid levels can give your doctor clues about your diagnosis.
· Urine tests. Analysis of your urine may show M proteins, which are referred to as Bence Jones proteins when they're detected in urine.
· Examination of your bone marrow. Your doctor may remove a sample of bone marrow for laboratory testing. The sample is collected with a long needle inserted into a bone (bone marrow aspiration and biopsy).
In the lab, the sample is examined for myeloma cells. Specialized tests, such as fluorescence in situ hybridization (FISH) can analyze myeloma cells to understand their chromosome abnormalities. Tests are also done to measure the rate at which the myeloma cells are dividing.
· Imaging tests. Imaging tests may be recommended to detect bone problems associated with multiple myeloma. Tests may include X-ray, MRI, CT or positron emission tomography (PET).
If tests indicate you have multiple myeloma, your doctor will use the information gathered from the diagnostic tests to classify your disease as stage 1, stage 2 or stage 3. Stage 1 indicates a less-aggressive disease and stage 3 indicates an aggressive disease that may affect bone, kidneys and other organs.
Your multiple myeloma may also be assigned a risk category, which indicates the aggressiveness of your disease.
Your multiple myeloma stage and risk category help your doctor understand your prognosis and your treatment options.
If you're experiencing symptoms, treatment can help relieve pain, control complications of the disease, stabilize your condition and slow the progress of the disease.
If you have multiple myeloma but aren't experiencing any symptoms (smoldering multiple myeloma), you may not need treatment. However, your doctor will regularly monitor your condition for signs the disease is progressing. This may involve periodic blood and urine tests.
If you develop signs and symptoms or your multiple myeloma shows signs of progression, you and your doctor may decide to begin treatment.
Though there's no cure for multiple myeloma, with good treatment results you can usually return to near-normal activity.
Standard treatment options include:
· Targeted therapy. Targeted drug treatment focuses on specific abnormalities within cancer cells that allow them to survive. Bortezomib (Velcade) and carfilzomib (Kyprolis) are targeted drugs that block the action of a substance in myeloma cells that breaks down proteins. This action causes myeloma cells to die. Both medications are administered through a vein in your arm.
· Biological therapy. Biological therapy drugs use your body's immune system to fight myeloma cells. The drugs thalidomide (Thalomid), lenalidomide (Revlimid) and pomalidomide (Pomalyst) enhance the immune system cells that identify and attack cancer cells. These medications are taken in pill form.
· Chemotherapy. Chemotherapy drugs kill fast-growing cells, including myeloma cells. Chemotherapy drugs can be given through a vein in your arm or taken in pill form. High doses of chemotherapy drugs are used before a stem cell transplant.
· Corticosteroids. Corticosteroids, such as prednisone and dexamethasone, regulate the immune system to control inflammation in the body. They also are active against myeloma cells. Corticosteroids can be taken in pill form or administered through a vein in your arm.
· Stem cell transplantation. A stem cell transplant is a procedure to replace your diseased bone marrow with healthy bone marrow.
Before a stem cell transplant, blood-forming stem cells are collected from your blood. You then receive high doses of chemotherapy to destroy your diseased bone marrow. Then your stem cells are infused into your body, where they travel to your bones and begin rebuilding your bone marrow.
· Radiation therapy. This treatment uses beams of energy, such as X-rays, to damage myeloma cells and stop their growth. Radiation therapy may be used to quickly shrink myeloma cells in a specific area — for instance, when a collection of abnormal plasma cells form a tumor (plasmacytoma) that's causing pain or destroying a bone.
Which combination of treatments you're likely to receive will depend on whether you're considered a good candidate for stem cell transplant. This depends on the risk of your disease progressing, your age and your overall health.
· If you're considered a candidate for stem cell transplant, your initial therapy will likely include a combination of treatments, such as targeted therapy, biological therapy, corticosteroids and, sometimes, chemotherapy.
Your stem cells will likely be collected after you've undergone a few months of treatment. You may undergo the stem cell transplant soon after your cells are collected or the transplant may be delayed until after a relapse, if it occurs. In some cases, doctors recommend two stem cell transplants for people with multiple myeloma.
After your stem cell transplant, you'll likely receive targeted therapy or biological therapy as a maintenance treatment to prevent a recurrence of myeloma.
· If you're not considered a candidate for stem cell transplant, your initial therapy will likely include chemotherapy combined with corticosteroids, targeted therapy or biological therapy.
In select cases, doctors use a reduced-intensity stem cell transplant in older people who are in very good health but can't tolerate the strong chemotherapy doses used in a traditional stem cell transplant. A reduced-intensity or "mini" stem cell transplant uses lower doses of chemotherapy.
· If your myeloma recurs or doesn't respond to treatment, your doctor may recommend repeating another course of the treatment that initially helped you. Another option is trying one or more of the other treatments typically used as first line therapy, either alone or in combination.
Research on a number of new treatment options is ongoing, and you may be eligible for a clinical trial in order to gain access to those experimental treatments. Talk to your doctor about what clinical trials may be available to you.
Because multiple myeloma can cause a number of complications, you may also need treatment for those specific conditions. For example:
· Bone pain. Pain medications, radiation therapy and surgery may help control bone pain.
· Kidney complications. People with severe kidney damage may need dialysis.
· Infections. Your doctor may recommend certain vaccines to prevent infections, such as the flu and pneumonia.
· Bone loss. Your doctor may recommend medications called bisphosphonates, such as pamidronate (Aredia) or zoledronic acid (Zometa), to help prevent bone loss.
· Anemia. If you have persistent anemia, your doctor may recommend medications to increase your red blood cell count.
No alternative medicines have been found to treat multiple myeloma. But alternative medicine may help you cope with the side effects of myeloma and myeloma treatment.
Talk to your doctor about your options, such as:
· Acupuncture
· Aromatherapy
· Massage
· Meditation
· Relaxation techniques
Talk with your doctor before trying any of these techniques to make sure they don't pose any risks for you.
A cancer diagnosis can be shocking and devastating. With time, you'll find ways to cope with the stress and uncertainty of living with cancer. Until you find what works best for you, consider trying to:
· Learn enough to make decisions about your care. Learn enough about multiple myeloma so that you can participate in making decisions about your treatment and care. Ask your doctor about your treatment options and their side effects.
You may find additional help gathering information through your local library and online. Start with the National Cancer Institute and the International Myeloma Foundation.
· Maintain a strong support system. Having a strong support system can help you cope with issues and anxieties that might occur. Your friends and family may be willing to offer support.
You might also find that support from a formal support group or others coping with cancer may be helpful. Friends you meet in support groups may be willing to share practical advice for coping with cancer and cancer treatment. Support groups are also available online.
· Set reasonable goals. Having goals helps you feel in control and can give you a sense of purpose. But don't choose goals you can't possibly reach. You may not be able to work a 40-hour week, for example, but you may be able to work at least part time. In fact, many people find that continuing to work during cancer treatment can be helpful in maintaining some normalcy.
· Take time for yourself. Eating well, relaxing and getting enough rest can help combat the stress and fatigue of cancer. Also, plan ahead for the downtimes when you may need to rest more or limit what you do.
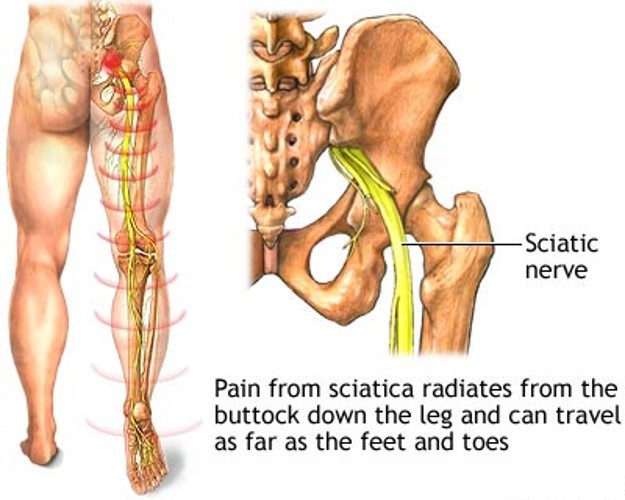
Sciatica refers to pain, weakness, numbness, or tingling in the leg. It is caused by injury to or pressure on the sciatic nerve. Sciatica is a symptom of another medical problem. It is not a medical condition on its own.
Sciatica occurs when there is pressure or damage to the sciatic nerve. This nerve starts in the lower back and runs down the back of each leg. This nerve controls the muscles of the back of the knee and lower leg. It also provides sensation to the back of the thigh, part of the lower leg, and the sole of the foot.
Sciatica pain can vary widely. It may feel like a mild tingling, dull ache, or burning sensation. In some cases, the pain is severe enough to make a person unable to move.
The pain most often occurs on one side. Some people have sharp pain in one part of the leg or hip and numbness in other parts. The pain or numbness may also be felt on the back of the calf or on the sole of the foot. The affected leg may feel weak. Sometimes, your foot gets caught on the ground when walking.
The pain often starts slowly. It may get worse:
· After standing or sitting
· At night
· When sneezing, coughing, or laughing
· When bending backward or walking more than a few yards, especially if caused by spinal stenosis
Because sciatica is a symptom of another medical condition, the underlying cause should be identified and treated.
In some cases, no treatment is required and recovery occurs on its own.
Conservative (non-surgical) treatment is best in many cases. Your doctor may recommend the following steps to calm your symptoms and reduce inflammation:
· Apply heat or ice to the painful area. Try ice for the first 48 to 72 hours, then use heat.
· Take over-the-counter pain relievers such as ibuprofen (Advil, Motrin IB) or acetaminophen (Tylenol).
· Reduce your activity for the first couple of days. Then, slowly start your usual activities.
· Do not do heavy lifting or twisting of your back for the first 6 weeks after the pain begins.
· Start exercising again after 2 to 3 weeks. Include exercises to strengthen your abdomen and improve flexibility of your spine.
Physical therapy may also be recommended. Additional treatments depend on the condition that is causing the sciatica.
If these measures do not help, your doctor may recommend injections of certain medicines to reduce swelling around the nerve. Other medicines may be prescribed to help reduce the stabbing pains due to nerve irritation.
Nerve pain is very difficult to treat. If you have ongoing problems with pain, you may want to see a neurologist or a pain specialist to ensure that you have access to the widest range of treatment options.
More serious complications depend on the cause of sciatica, such as slipped disc or spinal stenosis. Sciatica can lead to permanent numbness or weakness of your leg.
Toxic shock syndrome is caused by a toxin produced by certain types of Staphylococcus bacteria. A similar syndrome, called toxic shock-like syndrome (TSLS), can be caused by Streptococcal bacteria. Not all staph or strep infections cause toxic shock syndrome.
Although the earliest cases of toxic shock syndrome involved women who were using tampons during their periods (menstruation), today less than half of current cases are associated with such events. Toxic shock syndrome can also occur with skin infections, burns, and after surgery. The condition can also affect children, postmenopausal women, and men.
Risk factors include:
Recently having a baby
Staphylococcus aureus (S. aureus) infection, commonly called a Staph infection
Foreign bodies or packings (such as those used to stop nosebleeds)
Menstruation
Surgery
Tampon use (particularly if you leave one in for a long time)
Widespread red rash that looks like a sunburn -- skin peeling occurs 1 or 2 weeks after the rash, particularly on the palms of the hand or bottom of the feet
The diagnosis is based on several criteria: fever, low blood pressure, a rash that peels after 1-2 weeks, and problems with the function of at least three organs.
In some cases, blood cultures may be positive for growth of S. aureus.
Any foreign materials, such as tampons, vaginal sponges, or nasal packing, will be removed. Sites of infection (such as a surgical wound) will be drained.
The goal of treatment is to maintain important body functions. This may include:
Antibiotics for any infection (may be given through an IV)
Dialysis (if severe kidney problems are present)
Fluids through a vein (IV)
Medicines to control blood pressure
Intravenous gamma globulin in severe cases
Staying in the hospital intensive care unit (ICU) for monitoring
Toxic shock syndrome is a medical emergency. Seek immediate medical attention if you develop a rash, fever, and feel ill, particularly during menstruation and tampon use or if you have had recent surgery.
Menstrual toxic shock syndrome can be prevented by avoiding the use of highly absorbent tampons. You can reduce your risk by changing tampons more frequently and using tampons only once in a while (not regularly) during menstruation.
Инфекционно-токсический шок вызван токсином, вырабатываемым некоторыми видами бактерий стафилококка. Аналогичный синдром, называемый токсическим шоком - может быть вызван бактерией стрептококка. Не все стафилококковые или стрептококковые инфекции вызывают инфекционно-токсический шок.
Самые ранние случаи инфекционно-токсического шока возникали у женщин, использовавших тампоны во время месячных (менструации), сегодня же менее половины случаев заболевания связанны с подобными событиями. Инфекционно-токсический шок также может возникать при инфекциях кожи, ожогах и после операций. Заболевание может возникать у детей, женщин в постменопаузе и у мужчин.
Ни один метод обследования не может выявить инфекционно-токсический шок.
Диагноз основывается на нескольких критериях: лихорадка, низкое артериальное давление, сыпь, шелушение кожи через 1-2 недели после сыпи, а также проблемы с функционированием, по крайней мере, трех органов.
В некоторых случаях посев крови может выявить рост культуры золотистого стафилококка.
Любые инородные предметы и материалы, такие как тампоны, вагинальные губки или носовые тампоны должны быть удалены. Источник инфекции (например, хирургическая рана) должен быть очищен.
Цель лечения заключается в поддержании основных функций организма. Основные мероприятия:
Антибиотики для любой инфекции (могут быть введены внутривенно)
Диализ (при развитии почечной недостаточности)
Внутривенное введение жидкостей
Лекарственные препараты для контроля артериального давления
В тяжелых случаях внутривенное введение гамма-глобулина
Пребывание в отделении интенсивной терапии для мониторинга состояния
Инфекционно-токсический шок требует оказания неотложной медицинской помощи. Немедленно обратитесь к врачу, если у вас появились сыпь, лихорадка, чувство недомогания, особенно во время менструации и при использовании тампона, или если вам недавно была проведена хирургическая операция.
Менструальный инфекционно-токсический шок может быть предотвращен путем отказа от использования сильно впитывающих тампонов. Вы можете снизить риск путем частой замены тампонов и использования тампонов только один раз (не регулярно) за время менструации.
Fifth disease is an illness caused by a virus that leads to a rash on the cheeks, arms, and legs.
Causes
Fifth disease is caused by human parvovirus B19. It often affects preschoolers or school-age children during the spring. The disease is spread by contact with respiratory secretions.
The first sign of the disease is usually bright red cheeks, which look as though the child has been recently slapped on both sides of the face. Following this, a rash appears on the arms and legs and middle of the body. The rash fades from the center outwards, giving it a lacy appearance. Over a period of 1 to 2 weeks, the rash completely goes away.
Fifth disease is also sometimes associated with fever.
If a pregnant woman becomes infected with parvovirus B19, it can cause significant harm to her unborn baby. Any pregnant woman who believes that she may have been in contact with a person who has this virus should talk to her health care provider.
Parvovirus B19 is also thought to cause other diseases, including an infectious form of arthritis.
The majority of adults seem to have antibodies to parvovirus B19 in their bodies. This indicates that most people have been exposed to the virus, and also suggests that many infections go unnoticed.
Temporary anemia -- this is only serious if the patient has an immune system problem and some other, existing form of anemia
Exams and tests
Fifth disease causes a very distinct rash. Your health care provider will examine the appearance and pattern of the rash. This is usually all that is needed to make a diagnosis.
Blood tests that look for antibodies against parvovirus B19 may indicate infection. However, these tests are usually not needed, although they may be helpful in the diagnosis of aplastic crisis and persistent anemia.
Testing may also be done when there is a question of whether a pregnant woman has been exposed to the virus.
Treatment
No treatment is usually required for fifth disease in children. If fever or joint discomfort is present, then oral acetaminophen (such as Tylenol) may be given.
Outlook (prognosis)
Since this is a mild and generally benign viral infection, complete recovery can be expected.