Many diseases can cause malabsorption. Most often, malabsorption involves problems absorbing certain sugars, fats, proteins, or vitamins. It can also involve an overall problem with absorbing food.
Problems or damage to the small intestine that may lead to problems absorbing important nutrients. These include:
· Surgery that removes all or part of the small intestine
Enzymes produced by the pancreas help absorb fats and other nutrients. A decrease of these enzymes makes it harder to absorb fats and certain nutrients. Problems with the pancreas may be caused by:
In children, current weight or rate of weight gain is often much lower than that of other children of similar age and gender. This is called failure to thrive. The child may not grow and develop normally.
Adults may also have failure to thrive, with weight loss, muscle wasting, weakness, and even problems thinking.
Changes in the stools are often present, but not always.
Treatment depends on the cause and is aimed at relieving symptoms and ensuring the body receives enough nutrients.
A high-calorie diet may be tried. It should supply:
· Key vitamins and minerals, such as iron, folic acid, and vitamin B12
· Enough carbohydrates, proteins, and fats
If needed, injections of some vitamins and minerals or special growth factors will be given. Those with damage to the pancreas may need to take pancreatic enzymes. Your provider will prescribe these if necessary.
Medicines to slow down the normal movement of the intestine can be tried. This may allow food to remain in the intestine longer
If the body is not able to absorb enough nutrients, total parenteral nutrition (TPN) is tried. It will help you or your child get nutrition from a special formula through a vein in the body. Your provider will select the right amount of calories and TPN solution. Sometimes, you can also eat and drink while getting nutrition from TPN.
An intestinal obstruction is a blockage of the digestive tract that prevents the proper passage of food. Some intestinal obstructions are present at birth, while others are caused by such problems as hernias, abnormal scar tissue growth after an abdominal operation, and inflammatory bowel disease (IBD).
Malrotation is twisting of the intestines (or bowel) caused by abnormal development while a fetus is in utero, and can cause obstruction.
Some children with intestinal malrotation are born with other associated conditions, including:
· abnormalities of other organs, including the spleen or liver
Some kids with malrotation never experience complications and are never diagnosed. But most develop symptoms during infancy, and the majority are diagnosed by 1 year of age. Although surgery is required to repair malrotation, most kids will go on to grow and develop normally after treatment.
The small and large intestines are the longest part of the digestive system. If stretched out to their full length, they would measure more than 20 feet long by adulthood, but because they're folded up, they fit into the relatively small space inside the abdomen.
Malrotation occurs when the intestines don't position themselves normally during fetal development and aren't attached inside properly as a result. The exact reason this occurs is unknown.
When a fetus develops in the womb, the intestines start out as a small, straight tube between the stomach and the rectum. As this tube develops into separate organs, the intestines move into the umbilical cord, which supplies nutrients to the developing embryo.
Near the end of the first trimester of pregnancy, the intestines move from the umbilical cord into the abdomen. When they don't properly turn after moving into the abdomen, malrotation occurs.
Malrotation in itself may not cause any problems. However, it can lead to other complications:
· Bands of tissue called Ladd's bands may form, obstructing the first part of the small intestine (the duodenum).
· In a condition called volvulus, the bowel twists on itself, cutting off the blood flow to the tissue and causing the tissue to die. The symptoms associated with volvulus, including pain and cramping, are often what lead to the diagnosis of malrotation.
· Obstruction caused by volvulus or Ladd's bands is a potentially life-threatening problem. The bowel can stop functioning and intestinal tissue can die from lack of blood supply if an obstruction isn't recognized and treated. Volvulus, especially, is an emergency situation, with the entire small intestine in jeopardy.
One of the earliest signs of malrotation and volvulus is abdominal pain and cramping caused by the inability of the bowel to push food past the obstruction. When infants experience this cramping they may:
· pull up their legs and cry
· stop crying suddenly
· behave normally for 15 to 30 minutes
· repeat this behavior when the next cramp happens
Infants also may be irritable, lethargic, or have irregular stools.
Vomiting is another symptom of malrotation, and it can help the doctor determine where the obstruction is located. Vomiting that happens soon after the baby starts to cry often means the obstruction is in the small intestine; delayed vomiting usually means the blockage is in the large intestine. The vomit may contain bile (which is yellow or green in color) or may resemble feces.
Additional symptoms of malrotation and volvulus may include:
· a swollen abdomen that's tender to the touch
· diarrhea and/or bloody stools (or sometimes no stools at all)
· irritability or crying in pain, with nothing seeming to help
If volvulus or another intestinal blockage is suspected, the doctor will examine your child and then may order X-rays, a computed tomography (CT) scan, or an ultrasound of the abdominal area.
The doctor may use barium or another liquid contrast agent to see the X-ray or scan more clearly. The contrast can show if the bowel has a malformation and can usually determine where a blockage is located.
Adults and older kids usually drink barium in a liquid form. Infants may need to be given barium through a tube inserted from the nose into the stomach, or sometimes are given a barium enema, in which the liquid barium is inserted through the rectum.
Treating significant malrotation almost always requires surgery. The timing and urgency will depend on the child's condition. If there is already a volvulus, surgery must be performed right away in order to prevent damage to the bowel.
Any child with bowel obstruction will need to be hospitalized. A tube called a nasogastric(NG) tube is usually inserted through the nose and down into the stomach to remove the contents of the stomach and upper intestines. This keeps fluid and gas from building up in the abdomen. The child may also be given intravenous (IV) fluids to help prevent dehydration and antibiotics to prevent infection.
During the surgery, which is called a Ladd procedure, the intestine is straightened out, the Ladd's bands are divided, the small intestine is folded into the right side of the abdomen, and the colon is placed on the left side.
Because the appendix is usually found on the left side of the abdomen when there is malrotation (normally, the appendix is found on the right), it is removed. Otherwise, should the child ever develop appendicitis, it could complicate diagnosis and treatment.
If it appears that blood may still not be flowing properly to the intestines, the doctor may perform a second surgery within 48 hours of the first. If the bowel still looks unhealthy at this time, the damaged portion may be removed.
If the child is seriously ill at the time of surgery, an ileostomy or colostomy will usually be performed. In this procedure, the diseased bowel is completely removed, and the end of the normal, healthy intestine is brought out through an opening on the skin of the abdomen (called a stoma). Fecal matter passes through this opening and into a bag that is taped or attached with adhesive to the child's belly.
In young children, depending on how much bowel was removed, the ileostomy or colostomy is often a temporary condition that can later be reversed with another operation.
The majority of these surgeries are successful, although some kids have recurring problems after surgery. Recurrent volvulus is rare, but a second bowel obstruction due to adhesions (scar tissue build-up after any type of abdominal surgery) could occur later.
Children who require removal of a large portion of the small intestine can have too little bowel to maintain adequate nutrition (a condition known as short bowel syndrome). They may be dependent on intravenous nutrition for a time after surgery (or even permanently if too little intestine remains) and may require a special diet afterward.
Most kids in whom the volvulus and malrotation are identified early, before permanent injury to the bowel has occurred, do well and develop normally.
If you suspect any kind of intestinal obstruction because your child has bilious (yellow or green) vomiting, a swollen abdomen, or bloody stools, call your doctor immediately, and take your child to the emergency room right away.
Belching is the act of bringing up air from the stomach.
Considerations
Belching is most often a normal process. The purpose of belching is to release air from the stomach. Every time you swallow, you also swallow air, along with fluid or food.
The buildup of air in the upper stomach causes the stomach to stretch. This triggers the muscle at the lower end of the esophagus (the tube that runs from your mouth to the stomach) to relax. Air is allowed to escape up the esophagus and out the mouth.
Depending on the cause, belching may last longer or be more forceful.
Symptoms such as nausea, dyspepsia, and heartburn may be relieved by belching.
Causes
Belching may be due to:
· Pressure caused by the unconscious swallowing of air (aerophasia)
Диспепсия или нарушение переваривания пищи – это легкое ощущение дискомфорта в верхней части живота, возникающее во время или сразу после еды. Оно может ощущаться как:
Тепло, жжение или боль между пупком и нижней частью грудины
Неприятное чувство наполненности, которое возникает во время или сразу после приема пищи
В большинстве случаев диспепсия не является признаком серьезных проблем со здоровьем, если она не сочетается с другими симптомами, такими как кровотечение, потеря веса или проблемы с глотанием.
Изменение режима питания может помочь облегчить ваши симптомы. Шаги, которые можно предпринять:
Оставьте достаточное количество времени для приема пищи (не торопитесь)
Тщательно и полностью пережевывайте пищу
Старайтесь не разговаривать во время еды
Избегайте волнения или выполнения физической нагрузки сразу после еды
Расслабьтесь и отдохните, если нарушение переваривания вызвано стрессом
Избегайте приема аспирина и других НПВП. Если вы все же должны принять их, сделайте это на полный желудок.
Прием антацидов (препарат, нейтрализующий соляную кислоту, содержащуюся в желудочном соке) может облегчить диспепсию.
Такие лекарственные препараты, как ранитидин (Зантак) и омепразола (Прилосек) также могут облегчить симптомы. Врач может рекомендовать вам прием этих лекарств в больших дозах или в течение длительного периода времени.
Немедленно обратитесь за медицинской помощью, если вы чувствуете боль в челюсти, в груди, в спине, потливость, беспокойство или чувство обреченности. Это возможные симптомы сердечного приступа.
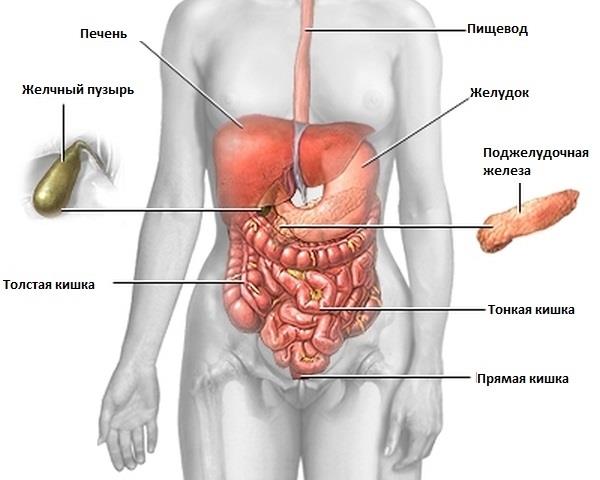
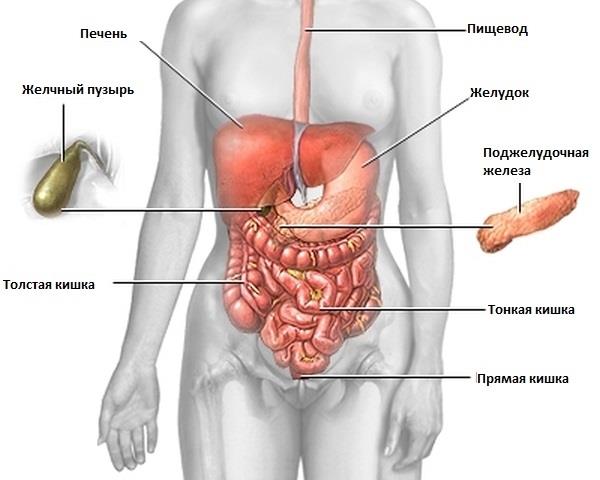
Поджелудочная железа располагается позади желудка и вырабатывает пищеварительные (энзимы) и гормональные ферменты, такие как инсулин и глюкагон. Активные энзимы (пищеварительные ферменты) поступают в просвет тонкой кишки и являются важным звеном в процессе переваривания пищи.
Острый панкреатит чаще возникает у мужчин, чем у женщин. Отдельные заболевания, оперативные вмешательства, пагубные привычки и неправильное питание увеличивают риск развития данного заболевания.
Заболевание чаще всего вызвано алкоголизмом и злоупотреблением алкоголем (в США -70% случаев). Также на развитие заболевания оказывает влияние генетический фактор. В других случаях причина остается неизвестной.
Ограничение употребления пищи для уменьшения нагрузки на поджелудочную железу
Иногда через нос или рот устанавливается назогастральный зонд (трубка), через который удаляется желудочное содержимое. Данный метод применяется в случае, если рвота или сильная боль ничем не купируется, или возможно развитие пареза кишечника (паралич кишечника). Зонд устанавливается на протяжении от 1 - 2 дней до 1 - 2 недель.
Газы, вздутие и неопределенный брюшной дискомфорт.
Частый понос и зловонный стул.
Слабость.
Потерю веса.
Ваш врач может оценить имеющиеся у Вас симптомы для выяснения причины и рекомендовать лечение.Лечение может включать специальную диету, медикаментозное лечение для замены кишечных ферментов и уменьшения спазмов, белково-минеральные добавки, такие как B12 и железо.
Незавершенный поворот кишечника это врожденный дефект, вызванный неправильным расположением кишечника плода в брюшном отделе, когда плод все ещё находится в матке. Незавершенный поворот кишечника может вызвать внезапное скручивание кишечника.
Большинство младенцев с незавершенным поворотом кишечника проявляют симптомы в течение первого месяца жизни.
Симптомы включают:
Рвоту кровью или зеленой жидкостью (желчь).
Вздутие живота.
Недостаточное питание.
Потерю веса.
Плач и обеспокоенность.
Необходимо немедленно обратиться в скорую медицинскую помощь в случае рвоты кровью или зеленой жидкостью.
Если имеются симптомы незавершенного поворота кишечника, обычно требуется хирургическое вмешательство для исправления положения кишечника.
Газы, отрыжка или вздутие живота, как правило, появляются после заглатывания воздуха, приема пищевых продуктов, вызывающих образование газов, или питья газированных напитков. Это нормально, и обычно их можно предотвратить, совершив кое-какие простые изменения.
Газы, отрыжка или вздутие живота после еды и питья также могут быть вызваны неспособностью:
Переваривать определенные разновидности сахара (например, лактозу, фруктозу или сорбит). Эти разновидности сахара часто добавляются к продовольственным продуктам и лекарствам, чтобы подсластить их. Лактозаобнаруживается в молоке, сыре и других молочных продуктах.
Правильно всасывать питательные вещества, витамины и минералы из пищеварительного тракта (синдроммальабсорбции). К причинам синдрома мальабсорбции относятся:
Отсутствие или низкие уровни определенных пищеварительных ферментов.
Заболевания, вызванные паразитами (лямблиоз, черви или амебиаз).
Изменения в бактериях, обычно обнаруживаемых в пищеварительном тракте.
Заболевания, поражающие саму кишку, например, глютеновая болезнь, которая часто развивается в детстве после добавления в пищу продуктов, содержащих глютен.
Операция, вследствие которой изменилась или сократилась длина желудочно-кишечного тракта.
Врач может проверить ваши симптомы для выявления их причины и порекомендует лечение. Лечение может включать изменения диеты, лекарства, заменяющие пищеварительные ферменты и способствующие уменьшению симптомов, а также питательные добавки (например, железо).