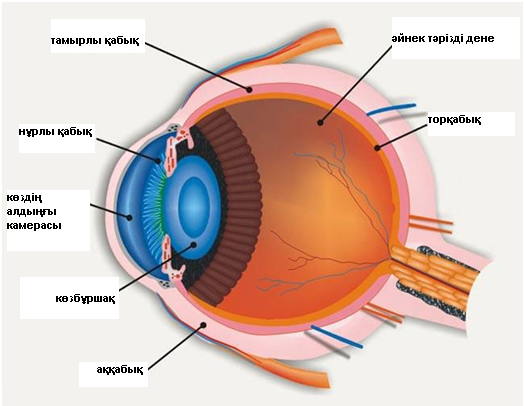
Көз ұясы үш қабықшадан және ішіндегілерден тұрады:
1) көздің сыртқы қабығы: аққабық (пішіні мен ширақтығын қамтамасыз ететін мөлдір емес бөлік), мөлдірқабық (жарық өтуі мен жарық сынуын қамтамасыз ететін мөлдір бөлік);
2) тамырлы қабық: нұрлы қабық (көзбұршақтың өлшемін реттейтін алдыңғы бөлігі), цилиарлық дене (көз ішілік сұйықтықты түзетін ортаңғы бөлік), хориоидея (торқабықты – көз түбін қоректендіретін артқы бөлік);
3) торқабық (өне бойымен ішкі жағымен әйнек тәрізді денеге жақын жататын көздің ішкі қабығы, ал сыртқы жағымен — тамырлы қабыққа жақын, алдыңғы көрмейтін бөліктен және біз көретін заттар бейнеленетін, артқы көретін бөліктен тұрады);
Көздің ішіндегісі: көзбұршақ (түрлі алыстағы заттарға көзді тоқтатуға-фокустеуге қатысатын биологиялық линза), әйнек тәрізді дене (мөлдір гель, көзбұршақты көз түбінен бөліп тұратын, көздің пішімін ұстап тұратын және жарық сәулесін торқабыққа өткізетін).
Торқабықтың ажырауы кенет пайда болып, көрмей қалуға апаруы мүмкін. Көбінесе, торқабықтың ажырауы орта және егде жастағы адамдарда пайда болады. алайда, бұл ауру балаларда, жаңа туған сәбилерде де болуы мүмкін.
· Алыстан көрмеудің орташа және жоғары дәрежесі (жақыннан жақсы көреді, алыстан нашар көреді) – бұл кезде көз ұясы ұзарады, торқабық созылады, шеттері жұқарады және үзіледі.
· Көздің жарақаты немесе офтальмологиялық операциялар.
· Қант диабетінде, қандағы қанттың деңгейі жоғары. Бұл қантамырларының зақымдануына апарады, оның ішінде, торқабықтың ұсақ тамырларының. Тамырлар жұқарады және жарылады, қан торқабықтың алдындағы бөлікке түседі, бұл көрудің бұзылуымен қосарланады. Қанның жиналуы тыртықтың түзілуіне апарады, олар торқабықты өзімен тартады, нәтижесінде, ол көздің тамырлы қабығынан ажырайды.
Торқабықтың ажырауы тек оперативтік тәсілмен емделеді.
· Криопексия (суықпен әсер ету) торқабықтың тұтастығын аурудың әр түрлі сатысында қалпына келтіруге қабілетті.
· Лазермен емдеу көздің торлы және тамырлы қабығының арасында бірігу түзілуі үшін қолданылады.
· Пневматикалық ретинопексия — хирургиялық емдеу тәсілі, ажыраудың кейбір түрінде тиімді. Бұл кезде әйнек тәрізді денеге көз ұясының ішіне ауа көпіршігін енгізеді, ол кеңейе отырып, торқабықты көздің қабырғасына қысады. Бұл шарадан кейін қосымша лазерлік емдеу қажет болады. 85% жағдайда пневматикалық ретинопексия көруді қалпына келтіреді.
· Склералау – склералық таңғыш аталатын арнайы силикон лентаны көз ұясын айналдыра орналастыру, бұл торқабықты «жабыстыруға» мүмкіндік береді. Склералық таңғыш (көздегі бандаж) торқабықты тамырлы қабыққа тығыздап, қысады және көрінбейді. Склералық лентаны орнатқаннан кейін оны қыздырумен жалғайды. Торқабықты склералаудың тиімділігі - 95% жуық.
· Витрэктомия – шағын тіліктер салу, олар арқылы әйнек тәрізді дене алынып, арнайы ерітінділермен алмастырылады. Витрэктомияның тиімділігі склералаудың тиімділігіне жуық.
Емдеудің табыстылығы торқабықты ажыраған тұсының орналасуына және емдеудің уақытылы болуына байланысты. Егер көздің макуласы (көрудің фокустелуіне жауап беретін бөлік) зақымданбаған болса, операциядан кейін көруді қалпына келтіру мүмкіндігі зор. Торқабықтың ажырауының көптеген түрлері емделеді, бәрі болмаса да. Операциядан кейін көру ішінара ғана қалпына келуі мүмкін.
· Күннен қорғайтын көзілдірік, көз жарақатын болдырмау үшін.
· Диабет кезінде қандағы қант деңгейін бақылау.
· Офтальмологқа бар, кемінде, жылына бір рет.
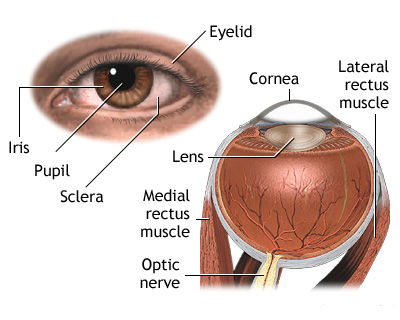
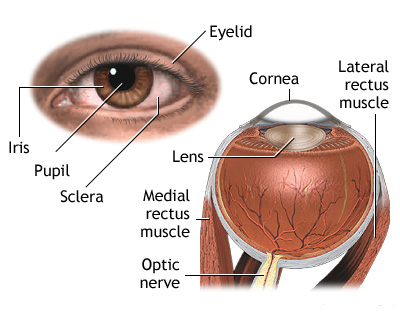
Retinal detachment is a separation of the light-sensitive membrane in the back of the eye (the retina) from its supporting layers.
CAUSES.
The most common type of retinal detachments are often due to a tear or hole in the retina. Eye fluids may leak through this opening. This causes the retina to separate from the underlying tissues, much like a bubble under wallpaper. This is most often caused by a condition called posterior vitreous detachment. However, it may also be caused by trauma and very bad nearsightedness. A family history of retinal detachment also increases your risk.
Another type of retinal detachment is called tractional detachment. This is seen in people who have uncontrolled diabetes, previous retinal surgery, or have chronic inflammation.
When the retina becomes detached, bleeding from area blood vessels may cloud the inside of the eye, which is normally filled with vitreous fluid. Central vision becomes severely affected if the macula, the part of the retina responsible for fine vision, becomes detached.
SYMPTOMS
Bright flashes of light, especially in peripheral vision
Most people with a retinal detachment will need surgery. Surgery may be done immediately or after a short period of time.
Surgery may not be needed if you do not have symptoms or have had the detachment for a while.
Some types of retinal detachment surgery can be done in your doctor's office.
Lasers may be used to seal tears or holes in the retina before a retinal detachment occurs.
If you have a small retinal detachment, the doctor may place a gas bubble in the eye. This is called pneumatic retinopexy. It helps help the retina float back into place. The hole is sealed with a laser.
More severe detachments may require surgery in a hospital operating room. Such procedures include:
Scleral buckle to gently push the eye wall up against the retina
Vitrectomy to remove gel or scar tissue pulling on the retina, used for the largest tears and detachments.
Tractional retinal detachments may be watched for a while before surgery. If surgery is needed, a vitrectomy is usually done.
PROGNOSIS
How well you do after a retinal detachment depends on the location and extent of the detachment and early treatment. If the macula was not damaged, the outlook with treatment can be excellent.
Most retinal detachments can be repaired, but not all of them. You may not get back all of your vision after surgery.
POSSIBLE COMPLICATIONS
A retinal detachment causes loss of vision. Surgery to repair it may help restore some or all of your vision.
WHEN TO CONTACT ВРАЧА
A retinal detachment is an urgent problem that requires medical attention within 24 hours of the first symptoms.
PREVENTION
Use protective eye wear to prevent eye trauma. Control your blood sugar carefully if you have diabetes. See your eye care specialist at least yearly, especially if you have risk factors for retinal detachment.
The structure of your face helps protect your eyes from injury. Still, injuries can damage your eye, sometimes severely enough that you could lose your vision. Most eye injuries are preventable. If you play sports or work in certain jobs, you may need protection.
The most common type of injury happens when something irritates the outer surface of your eye. Certain jobs such as industrial jobs or hobbies such as carpentry make this type of injury more likely. It's also more likely if you wear contact lenses.
Chemicals or heat can burn your eyes. With chemicals, the pain may cause you to close your eyes. This traps the irritant next to the eye and may cause more damage. You should wash out your eye right away while you wait for medical help.
A chalazion is a small bump in the eyelid caused by a blockage of a tiny oil gland.
Causes
A chalazion is caused by a blocked duct in one of the Meibomian glands. These glands are located in the eyelid directly behind the eyelashes and produce a thin, oily fluid that lubricates the eye.
Symptoms
A chalazion often develops after an internal hordeolum (another word for hordeolum is stye). The eyelid usually becomes tender, red, swollen and warm. Sometimes, the blocked gland causing the stye will not drain even though the redness and swelling goes away. The gland will form a firm, non-tender nodule in the eyelid which is called a chalazion.
Exams and Tests
An exam of the eyelid confirms the diagnosis.
Rarely, skin cancer of the eyelid may look like a chalazion. If this is suspected, you may need a biopsy.
Treatment
A chalazion will often disappear without treatment in a month or so.
The first treatment is to place warm compresses over the eyelid for 10-15 minutes at least four times a day. Use water that is no hotter than you can leave your hand in comfortably. This may soften the hardened oils blocking the duct, and promote drainage and healing.
Do not push or squeeze the chalazion.
If the chalazion continues to get bigger, it may need to be removed with surgery. This is most often done from the inside of the eyelid to avoid a scar on the skin.
Chalazia usually heal on their own. The outcome with treatment is usually excellent.
Possible Complications
Rarely, a chalazion will heal by itself but may leave a scar on the eyelid. This problem is more common after chalazion surgery, but is still rare. You may lose some eyelashes or you may have a small notch in the edge of the eyelid. The most common complication is a return of the problem.
When to Contact a Medical Professional
Call your health care provider if lumps on the eyelid continue to get bigger despite treatment, or you have an area of eyelash loss.
Prevention
To prevent chalazia or styes, it may help to gently scrub the edge of the lid at the eyelash line nightly. Use eye cleansing pads or diluted baby shampoo.
Apply antibiotic ointment prescribed by your health care provider after scrubbing the eyelids.