Priapism is a prolonged erection of the penis. The unwanted, persistent erection isn't caused by sexual stimulation or arousal, and priapism is usually painful.
Priapism is an uncommon condition that needs immediate medical attention. Prompt treatment for priapism is usually needed to prevent tissue damage that could result in the inability to get or maintain an erection (erectile dysfunction).
Priapism is most common between ages 5 and 10 in boys and ages 20 and 50 in men.
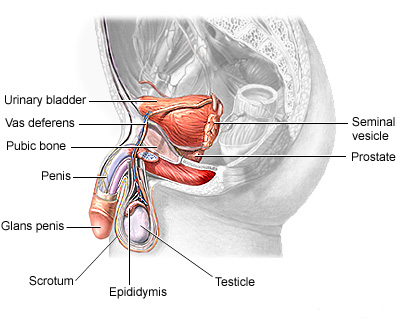
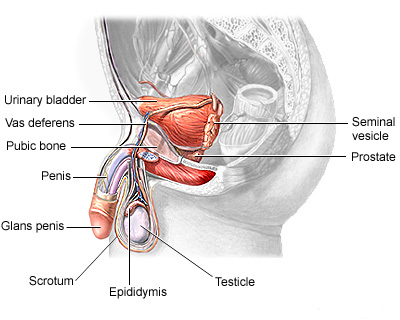
Male reproductive system
Priapism causes abnormally persistent erections not related to sexual stimulation. Priapism symptoms may vary depending on the type of priapism. There are two main types: ischemic and nonischemic priapism.
Ischemic priapism
Ischemic, also called low-flow, priapism is the result of blood not being able to leave the penis. It's the more common type of priapism. Signs and symptoms include:
Unwanted erection lasting more than four hours
Unwanted erection off and on for several hours (stuttering priapism)
Rigid penile shaft, but usually soft tip of penis (glans)
Usually painful or tender penis
Nonischemic priapism
Nonischemic, or high-flow, priapism occurs when too much blood flows into the penis. Nonischemic priapism is usually painless. Signs and symptoms include:
Unwanted erection lasting at least four hours
Erect but not rigid penile shaft
When to see a doctor
If you have an erection lasting longer than four hours, go to the emergency room. If you experience a painful, persistent erection that resolves on its own in less than four hours, see your doctor. You may need treatment to prevent further episodes.
An erection normally occurs in response to physical or psychological stimulation. This stimulation causes certain blood vessels to relax and expand, increasing blood flow to spongy tissues in the penis. Consequently, the blood-filled penis becomes erect. After stimulation ends, the blood flows out, and the penis returns to its nonrigid (flaccid) state.
Priapism occurs when some part of this system — the blood, blood vessels or nerves — changes normal blood flow. Subsequently, an unwanted erection persists. Factors that can contribute to priapism include the following.
Blood disorders, such as Leukemia
Prescription medications, such as antidepressants, blood thinners
Alcohol and drug use
Injury
Other factors, such as Blood clots, Spinal cord injury
In some cases, doctors are unable to identify the specific cause for priapism.
Ischemic priapism can cause serious complications. The blood trapped in the penis is deprived of oxygen. When an erection lasts for longer than four hours, this oxygen-poor blood can begin to damage or destroy tissues in the penis. As a result, untreated priapism may cause:
Erectile dysfunction, the inability of the penis to become or stay erect with sexual arousal
Disfigurement of the penis
If you or your child has experienced a painful, persistent erection that lasted less than four hours, or multiple unwanted, persistent erections (stuttering priapism), see your primary care doctor. If the erection has lasted more than four hours, go to the emergency room.
Your doctor or the emergency room doctor may suggest that you make a follow-up appointment with a specialist in reproductive and urinary organs (urologist).
If you have time before you see your doctor, it's a good idea to prepare for questions the doctor is likely to ask.
What you can do
Write down the symptoms, including any that may seem unrelated to the persistent erections.
Make a list of all medications, as well as any vitamins or supplements, that you're taking. And, let your doctor know if you've taken any nutritional supplements or illegal drugs.
You may also want to prepare a list of questions to ask the doctor:
What is likely causing the persistent erections?
What kind of tests might be needed?
What can be done to prevent this problem in the future?
If medication is necessary, is there a generic alternative?
Are there activities, such as exercise or sex, that should be avoided? If so, for how long?
Does priapism increase the risk of developing erectile dysfunction?
Do you have brochures or can you suggest websites that explain more about priapism?
If other questions occur to you or you don't understand something, don't hesitate to ask questions during your appointment.
What to expect from your doctor
Your doctor is likely to ask a number of questions regarding recurring episodes of persistent erections. Your doctor may ask:
When did your symptoms first start?
How long have the erections lasted?
Were the erections painful?
Have you had an injury to your genitals or groin?
Did the unwanted erections occur after using a particular substance, such as alcohol, marijuana, cocaine or other drugs?
Do you take any prescription medications, including drugs for treating erectile dysfunction? Do you take any herbal or dietary supplements?
Your doctor may also order laboratory tests to determine if a disease or condition is causing priapism.
What you can do in the meantime
Don't stop your prescription medications without consulting your doctor. Don't use any recreational substance that could cause persistent erections.
If you have an erection lasting more than four hours, you need emergency care. The emergency room doctor will determine first whether you have ischemic priapism or nonischemic priapism. This is necessary because the treatment for each is different, and treatment for ischemic priapism needs to be done as soon as possible.
Medical history and exam
To determine what type of priapism you have, your doctor will likely ask numerous questions and examine your genitals, abdomen, groin and perineum. He or she may be able to determine what type of priapism you have based on the rigidity and sensitivity of the penis. This exam may also reveal signs of injury or tumors that could be causing priapism. An injury, for example, would suggest that nonischemic priapism is more likely.
Diagnostic tests
Diagnostic tests may be necessary to determine what type of priapism you have. Additional tests may identify the cause of priapism. In an emergency room setting, your treatment may begin before all test results are received if the doctor is confident about what kind of priapism you have. Diagnostic tests include:
Blood gas measurement. In this test, a tiny needle is inserted into your penis to remove a sample of blood. If the blood is dark — deprived of oxygen — the condition is most likely ischemic priapism. If it's bright red, the priapism is most likely nonischemic. A laboratory test measuring the amounts of certain gases in the blood can confirm the type of priapism.
Blood tests. Your blood can be tested to measure the number of red blood cells and platelets present. Results may provide evidence of diseases, such as sickle cell anemia, other blood disorders or certain cancers.
Ultrasound. You may have color duplex ultrasonography, which uses sound waves to create an image of internal organs. This test can be used to measure blood flow within your penis that would suggest ischemic or nonischemic priapism. The exam may also reveal an injury, tumor or abnormality that may be an underlying cause.
Toxicology test. Your doctor may order a test to screen for illegal or prescription drugs that may be the cause of priapism. This test may be done with blood or urine samples.
Ischemic priapism
Ischemic priapism — the result of blood not being able to exit the penis — is an emergency situation that requires immediate treatment. This treatment usually begins with a combination of draining blood from the penis and using medications.
Aspiration. After your penis is numbed with local anesthetic, excess blood is drained from it, using a small needle and syringe. As part of this procedure, the penile veins may also be flushed with a saline solution. This treatment relieves pain, removes oxygen-poor blood and may stop the erection. This treatment may be repeated until the erection ends.
Medication. A medication called an alpha-adrenergic sympathomimetic, such as phenylephrine, may be injected into the spongy tissue of the penis. This drug constricts blood vessels that carry blood into the penis. This action allows blood vessels that carry blood out of the penis to open up and allow increased blood flow out. This treatment may be repeated over several hours if necessary. There is some risk of side effects, such as headache, dizziness and high blood pressure, particularly if you have high blood pressure or heart disease.
Surgery. If other treatments aren't successful, a surgeon may implant a device that reroutes blood flow (a shunt) so that blood can move through your penis normally.
Additional treatments. If you have sickle cell anemia, you may receive additional treatments that are used to treat disease-related episodes, such as supplemental oxygen or an intravenous solution to keep you hydrated.
Nonischemic priapism
Nonischemic priapism often goes away with no treatment. Because there isn't a risk of damage to the penis, your doctor may suggest a watch-and-wait approach. Putting ice and pressure on the perineum — the region between the base of the penis and the anus — may help end the erection.
Surgery may be necessary in some cases to insert material that temporarily blocks blood flow to the penis. The body eventually absorbs the material. Surgery may also be necessary to repair arteries or tissue damage resulting from an injury.
Depending on the probable cause of the priapism, steps to prevent recurrent priapism may include:
Treating the disease that may have caused priapism
Changing medications if a prescription medication was the probable cause
Avoiding triggers, such as alcohol or illegal drugs
Self-injection of phenylephrine to stop prolonged erections
An erection problem is when a man cannot get or keep an erection that is firm enough to have intercourse. You may be unable to get an erection at all. Or, you may lose the erection during intercourse before you are ready.
If the condition continues, it is called erectile dysfunction.
Erection problems are common in adult men. Almost all men sometimes have trouble getting or keeping an erection.
In many cases, the problem goes away with little or no treatment. In other cases, it can be an ongoing problem. If you have trouble getting or keeping an erection more than 25% of the time, it is a problem.
An erection problem that does not go away can damage your self-esteem and harm your relationship with your partner. It needs to be treated.
In the past, erection problems were thought to be "all in the man's mind." Men often were given unhelpful advice such as, "don't worry," or "just relax and it will take care of itself." Today, doctors believe that physical factors often cause erection problems.
One way to know if the cause is physical is whether you have nighttime erections. Normally, men have 3 to 5 erections per night. Each erection lasts for up to 30 minutes. Your doctor can tell you how to find out whether you are having the normal number of nighttime erections. If you have erections in the morning, this can also mean that there is not a physical cause.
Erection problems usually do not affect a man's sex drive.
Having an orgasm too quickly (premature ejaculation) is not the same as impotence. Get counseling with your partner for this problem.
Male infertility is also different from impotence. A man who cannot keep an erection may be able to produce sperm that can fertilize an egg. A man who is infertile can usually keep an erection, but he may not be able to father a child due to problems with sperm.
An erection involves your brain, nerves, hormones, and blood vessels. Anything that interferes with these normal functions can lead to problems getting an erection.
Common causes of erection problems include:
Diseases such as diabetes, high blood pressure, heart or thyroid conditions, poor blood flow, depression, or nervous system disorders (such as multiple sclerosis or Parkinson's disease)
Medicines, including blood pressure medications (especially beta-blockers), heart medications (such as digoxin), some peptic ulcer medications, sleeping pills, and antidepressants
Nerve damage from prostate surgery
Nicotine, alcohol, or cocaine use
Poor communication with your partner
Repeated feelings of doubt and failure
Spinal cord injury
Stress, fear, anxiety, or anger
Unrealistic sexual expectations, which make sex a task instead of a pleasure
Erection problems become more common with age. However, they can affect men at any age. Physical causes are more common in older men. Emotional causes are more common in younger men.
Low levels of testosterone can lead to erection problems. They may also reduce a man's sex drive.
Cut down on smoking, alcohol, and illegal drug use.
Get plenty of rest and take time to relax.
Exercise and eat a healthy diet to keep good blood circulation.
Use safe sex practices to prevent HIV and STDs.
Talk openly to your partner about sex and your relationship. If you cannot do this, counseling can help.
Couples who cannot talk to each other are likely to have problems with sexual intimacy. Men who have trouble talking about their feelings may find it hard to share their anxiety about sexual performance. Counseling can help both you and your partner.
The problem does not go away with lifestyle changes
The problem begins after an injury or prostate surgery
You have other symptoms, such as low back pain, abdominal pain, or a change in urination
If erection problems seem to be caused by a medication you are taking, talk to your health care provider. You may need to lower the dose or change to another drug. Do NOT change or stop taking any medications without first talking to your health care provider.
Talk to your health care provider if your erection problems have to do with a fear of heart problems. Sexual intercourse is usually safe for men with heart problems.
Call your doctor right away or go to an emergency room if the medication you are taking for erection problems gives you an erection that lasts for more than 4 hours.
Nocturnal penile tumescence (NPT) to check for normal nighttime erections
Penile ultrasound to check for blood vessel or blood flow problems
Psychometric testing
Rigidity monitoring
Urine analysis
TREATMENT
The treatment may depend on the cause of the problem. Talk to your health care provider about the best way to treat your erection problem.
There are many treatment options today, including:
Injections into the penis
Medicines inserted into the urethra
Medicines taken by mouth
Surgery
Vacuum devices
Ask your health care provider about the possible side effects and complications of each treatment.
Sildenafil (Viagra), vardenafil (Levitra), and tadalafil (Cialis) are medicines called phosphodiesterase-5 (PDE5) inhibitors. They work only when you are sexually aroused. They usually start to work in 15 to 45 minutes.
These drugs can have side effects, which can range from muscle pain and flushing to heart attack. Do not use these drugs with medications such as nitroglycerin. The combination can cause your blood pressure to drop. Some men have died after taking these drugs with nitroglycerin.
Use PDE5 inhibitors with caution if you have any of the following conditions:
If pills do not work, other treatment options include:
Testosterone replacement using skin patches, gel, or injections into the muscle -- if your testosterone level is low.
A medicine called alprostadil, injected into the penis or inserted into the urethra, improves blood flow to the penis. This usually works better than medications taken by mouth.
A vacuum device can be used to pull blood into the penis. A special rubber band is then used to keep the erection during intercourse.
Many herbs and dietary supplements are marketed to help sexual performance or desire. However, none of these supplements have been proven effective for treating erectile dysfunction, and they may not always be safe.