Which form of birth control you choose depends on a number of different factors, including your health, how often you have sex, and whether or not you want children.
Here are some factors to consider when selecting a birth control method:
Effectiveness -- How well does the method prevent pregnancy? Look at the number of pregnancies in 100 women using that method over a period of 1 year. If an unplanned pregnancy would be viewed as potentially devastating to the individual or couple, a highly effective method should be chosen. In contrast, if a couple is simply trying to postpone pregnancy, but feels that a pregnancy could be welcomed if it occurred earlier than planned, a less effective method may be a reasonable choice.
Cost -- is the method affordable?
Health risk -- What are the potential health risks? For example, birth control pills are usually not recommended for women over age 35 who also smoke.
Partner involvement -- The willingness of a partner to accept and support a given method may affect your choice of birth control. However, you also may want to reconsider a sexual relationship with a partner unwilling to take an active and supportive role.
Permanence -- Do you want a temporary (and generally less effective) method, or a long-term or even permanent (and more effective) method?
Preventing HIV and sexually transmitted infections (STIs) -- Many methods offer no protection against STIs. In general, condoms are the best choice for preventing STIs, especially when combined with spermicides.
Availability -- Can the method be used without a prescription, provider visit, or, in the case of minors, parental consent?
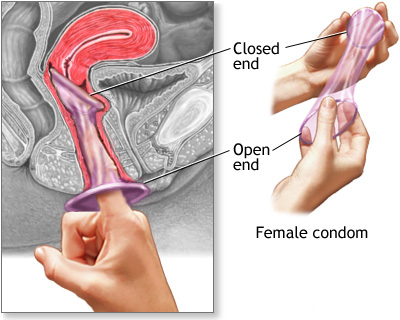
A condom is a thin latex or polyurethane sheath. The male condom is placed around the erect penis. Thefemale condom is placed inside the vagina before intercourse.
A condom must be worn at all times during intercourse to prevent pregnancy.
Condoms are available in most drug and grocery stores. Some family planning clinics offer free condoms. You do not need a prescription to get condoms.
The female condom, like the male condom, is a barrier contraceptive made of latex or polyurethane. The condom has a ring on each end. The ring that is placed inside the vagina fits over the cervix, while the other ring, which is open, rests outside of the vagina and covers the vulva. The female condom is sold over-the-counter.
Diaphragm and cervical cap
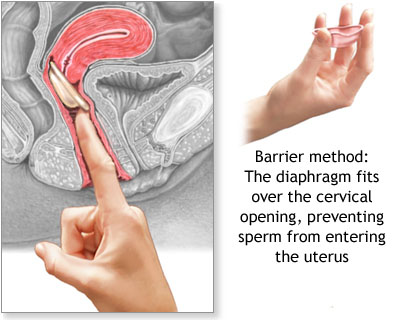
A diaphragm is a flexible rubber cup that is filled with spermicidal cream or jelly.
It is placed into the vagina over the cervix before intercourse, to prevent sperm from reaching the uterus.
It should be left in place for 6 to 8 hours after intercourse.
Diaphragms must be prescribed by a woman's health care provider, who determines the correct type and size of diaphragm for the woman.
About 5-20 pregnancies occur over 1 year in 100 women using this method, depending on proper use.
A similar, smaller device is called a cervical cap.
Risks include irritation and allergic reactions to the diaphragm or spermicide, and increased frequency of urinary tract infection. In rare cases, toxic shock syndrome may develop in women who leave the diaphragm in too long. A cervical cap may cause an abnormal Pap test.
A diaphragm is a flexible rubber cup that is filled with spermicide and self-inserted over the cervix prior to intercourse. The device is left in place several hours after intercourse. The diaphragm is a prescribed device fitted by a health care professional and is more expensive than other barrier methods such as condoms.
Vaginal sponge
Vaginal contraceptive sponges are soft synthetic sponges saturated with a spermicide. Prior to intercourse, the sponge is moistened, inserted into the vagina, and placed over the cervix.
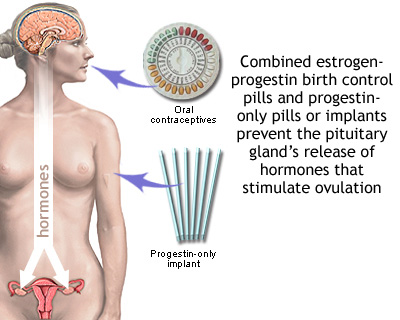
Birth control methods that use hormones will have either both an estrogen and a progestin, or a progestin alone.
Both hormones prevent a woman's ovary from releasing an egg during her menstrual cycle (called ovulation). They do this by affecting the levels of other hormones the body makes.
Progestins help prevent sperm from entering the uterus by making mucus around a woman's cervix thick and sticky.
The pill works in several ways to prevent pregnancy. The pill suppresses ovulation so that an egg is not released from the ovaries, and changes the cervical mucus, causing it to become thicker and making it more difficult for sperm to swim into the womb. The pill also does not allow the lining of the womb to develop enough to receive and nurture a fertilized egg.
This method of birth control offers no protection against sexually-transmitted diseases.
Types of hormonal birth control methods include:
Combination birth control pills, which combine the hormones estrogen and progestin to prevent ovulation.
Progestin only birth control pills, also called the "mini-pill."
Implants -- small rods implanted surgically beneath the skin, which release a continuous dose of progestin to prevent ovulation.
Progestin injections, such as Depo-Provera, are given into the muscles of the upper arm or buttocks once every 3 months. This injection prevents ovulation.
The skin patch (Ortho Evra) is placed on your shoulder, buttocks, or other convenient location. It continually releases progestin and estrogen. Like other hormone methods, a prescription is required.
The vaginal ring (NuvaRing) is a flexible ring about 2 inches wide that is placed into the vagina. It releases the hormones progestin and estrogen.
The IUD is a small plastic or copper device placed inside the woman's uterus by her health care provider. Some IUDs release small amounts of progestin. IUDs may be left in place for 5 - 10 years, depending on the device used.
IUDs can be placed at almost any time.
IUDs are safe and work well. Fewer than 1 out of 100 women per year will get pregnant using an IUD.
Risks and complications include cramps, bleeding (sometimes severe), and perforation of the uterus.
The progestin IUD often causes irregular spotting for the first several months. In about 50% of women, the periods may stop completely by the end of the first year. This effect goes away when the device is removed.
These methods are best for men, women, and couples who believe they never wish to have children in the future. While viewed as a permanent method, these operations can sometimes be reversed if a man or woman later chooses to become pregnant.
Coitus interruptus is the withdrawal of the penis from the vagina before ejaculation. Some semen frequently escapes before full withdrawal and before ejaculation, which is enough to cause a pregnancy.
Douching shortly after sex is ineffective because sperm can make their way past the cervix within 90 seconds after ejaculation.
Breastfeeding. Despite the myths, women who are breastfeeding can become pregnant.
An erection problem is when a man cannot get or keep an erection that is firm enough to have intercourse. You may be unable to get an erection at all. Or, you may lose the erection during intercourse before you are ready.
If the condition continues, it is called erectile dysfunction.
Erection problems are common in adult men. Almost all men sometimes have trouble getting or keeping an erection.
In many cases, the problem goes away with little or no treatment. In other cases, it can be an ongoing problem. If you have trouble getting or keeping an erection more than 25% of the time, it is a problem.
An erection problem that does not go away can damage your self-esteem and harm your relationship with your partner. It needs to be treated.
In the past, erection problems were thought to be "all in the man's mind." Men often were given unhelpful advice such as, "don't worry," or "just relax and it will take care of itself." Today, doctors believe that physical factors often cause erection problems.
One way to know if the cause is physical is whether you have nighttime erections. Normally, men have 3 to 5 erections per night. Each erection lasts for up to 30 minutes. Your doctor can tell you how to find out whether you are having the normal number of nighttime erections. If you have erections in the morning, this can also mean that there is not a physical cause.
Erection problems usually do not affect a man's sex drive.
Having an orgasm too quickly (premature ejaculation) is not the same as impotence. Get counseling with your partner for this problem.
Male infertility is also different from impotence. A man who cannot keep an erection may be able to produce sperm that can fertilize an egg. A man who is infertile can usually keep an erection, but he may not be able to father a child due to problems with sperm.
An erection involves your brain, nerves, hormones, and blood vessels. Anything that interferes with these normal functions can lead to problems getting an erection.
Common causes of erection problems include:
Diseases such as diabetes, high blood pressure, heart or thyroid conditions, poor blood flow, depression, or nervous system disorders (such as multiple sclerosis or Parkinson's disease)
Medicines, including blood pressure medications (especially beta-blockers), heart medications (such as digoxin), some peptic ulcer medications, sleeping pills, and antidepressants
Nerve damage from prostate surgery
Nicotine, alcohol, or cocaine use
Poor communication with your partner
Repeated feelings of doubt and failure
Spinal cord injury
Stress, fear, anxiety, or anger
Unrealistic sexual expectations, which make sex a task instead of a pleasure
Erection problems become more common with age. However, they can affect men at any age. Physical causes are more common in older men. Emotional causes are more common in younger men.
Low levels of testosterone can lead to erection problems. They may also reduce a man's sex drive.
Cut down on smoking, alcohol, and illegal drug use.
Get plenty of rest and take time to relax.
Exercise and eat a healthy diet to keep good blood circulation.
Use safe sex practices to prevent HIV and STDs.
Talk openly to your partner about sex and your relationship. If you cannot do this, counseling can help.
Couples who cannot talk to each other are likely to have problems with sexual intimacy. Men who have trouble talking about their feelings may find it hard to share their anxiety about sexual performance. Counseling can help both you and your partner.
The problem does not go away with lifestyle changes
The problem begins after an injury or prostate surgery
You have other symptoms, such as low back pain, abdominal pain, or a change in urination
If erection problems seem to be caused by a medication you are taking, talk to your health care provider. You may need to lower the dose or change to another drug. Do NOT change or stop taking any medications without first talking to your health care provider.
Talk to your health care provider if your erection problems have to do with a fear of heart problems. Sexual intercourse is usually safe for men with heart problems.
Call your doctor right away or go to an emergency room if the medication you are taking for erection problems gives you an erection that lasts for more than 4 hours.
Nocturnal penile tumescence (NPT) to check for normal nighttime erections
Penile ultrasound to check for blood vessel or blood flow problems
Psychometric testing
Rigidity monitoring
Urine analysis
TREATMENT
The treatment may depend on the cause of the problem. Talk to your health care provider about the best way to treat your erection problem.
There are many treatment options today, including:
Injections into the penis
Medicines inserted into the urethra
Medicines taken by mouth
Surgery
Vacuum devices
Ask your health care provider about the possible side effects and complications of each treatment.
Sildenafil (Viagra), vardenafil (Levitra), and tadalafil (Cialis) are medicines called phosphodiesterase-5 (PDE5) inhibitors. They work only when you are sexually aroused. They usually start to work in 15 to 45 minutes.
These drugs can have side effects, which can range from muscle pain and flushing to heart attack. Do not use these drugs with medications such as nitroglycerin. The combination can cause your blood pressure to drop. Some men have died after taking these drugs with nitroglycerin.
Use PDE5 inhibitors with caution if you have any of the following conditions:
If pills do not work, other treatment options include:
Testosterone replacement using skin patches, gel, or injections into the muscle -- if your testosterone level is low.
A medicine called alprostadil, injected into the penis or inserted into the urethra, improves blood flow to the penis. This usually works better than medications taken by mouth.
A vacuum device can be used to pull blood into the penis. A special rubber band is then used to keep the erection during intercourse.
Many herbs and dietary supplements are marketed to help sexual performance or desire. However, none of these supplements have been proven effective for treating erectile dysfunction, and they may not always be safe.