Метаболикалық синдром - жүрек-қан тамырлары ауруларының, инсульттің және 2 типті қант диабеттің пайда болу қаупін арттыратын қауіп-қатер факторларының топтары.
Себептері
Ғалымдар әлі де метаболикалық синдромның қандай да бір себептермен пайда болатынына сенімді емес. Дегенмен, бұл синдроммен байланысты барлық қауіп-қатерлер семіздікпен немесе жай артық салмақпен байланысты екені белгілі.
Метоболикалық синдромның ең негізгі қауіп-қатер факторлары:
Дененің ортаңғы және жоғарғы бөліктерінде артық салмақтың жиналуынан (орталық семіру), денені «алма тәрізді» деп сипаттауға болады.
Инсулинге төзімділік. Дене инсулинді қалыпты жағдайға қарағанда төмен пайдаланады. Инсулин ағзадағы қантты бақылау үшін қажет. Инсулинді тиімсіз пайдаланудың нәтижесінде, ағзадағы қант пен майдың мөлшері артады.
Басқа қауіп-қатер факторына жатады:
Жасы
Метаболикалық синдромның пайда болуына генетикалық бейімділік
Гормоналды өзгерістер
Физикалық белсенділіктің жеткіліксіздігі
Метаболикалық синдромнан зардап шегетін адамдарда, аурудың ағымын нашарлататыннемесе осыаурудың себебі болуы мүмкінбасқа да қиындықтарболады, және олар келесі салдарға алып келеді:
Қанның шамадан тыс ұюы
Ағзадағы қабыну белгісін көрсететін заттардың қанда жоғарылауы
Диагностикасы
Науқас метаболикалық синдромнан зардап шегеді, егер төменде көрсетілген үш немесе одан да көп симптомдар болса:
Қан қысымы 130/85 мм сын.бағ. жоғары
Аш қарынға қандағы қанттың деңгейі 100 мг / дл жоғары
Үлкен бел айналымы:
Ерлерде – 100 сантиметрден жоғары
Әйелдерде – 88 сантиметрден жоғары
Жоғарғы тығыздықты липопротеиндердің құрамындағы холестерин деңгейінің төмен болуы
Ерлерде – 40 мг/длтөмен
Әйелдерде – 50 мг/длтөмен
Триглицеридтердің деңгейі 150 мг / длжоғары
Емі
Емдеудің мақсаты - жүрек аурулары мен қант диабетінің пайда болу қаупін азайту. Емдеуші дәрігер науқасқа өмір сүру салтын өзгертуді және қан қысымын, ЖТЛП холестеринді, қандағы қант деңгейін төмендетуге арналған дәрі-дәрмектерді ұсынуы мүмкін.
Артық салмақтан арылу. Метаболикалық синдроммен зардап шегетін адам салмақтың 7-10 пайызын тастау керек. Бір күнде 500-1000 калорияға аз тамақтану керек.
Орташа қарқынды физикалық жаттығулар үшін кем дегенде 30 минут уақытын бөлу керек, мысалы, аптасына 5-7 рет серуендеу қажет.
Арықтау, физикалық белсенділік және холестериннің деңгейін төмендету үшін арналған препараттарды қолдану арқылы қандағы холестерин деңгейін төмендету керек.
Арықтау, физикалық жаттығулар немесе дәрілік препараттар арқылы қан қысымының деңгейін төмендету керек.
Шылым шегетін адамдар зиянды әдеттерін тастауы керек.
Ағымы
Метаболикалық синдромы бар адамдарда жүрек ауруына, 2-ші типтегі диабетке, инсультке, бүйрек ауруларына шалдығу қаупі жоғары болады және аяқтарының қандануы жеткіліксіз болуы мүмкін.
Дәрігерге қашан қаралу керек
Егер сізде осы аурудың белгілері немесе симптомдары болса дәрігерге қаралыңыз.
Аударған: Дүйсенова Жаңылсын Бекқалиқызы
Мазмұны
Жалпы ақпарат
Себептері
Симптомдар
Диагностика
Емі
Болжамы
Дәрігерге қашан қаралу керек?
Жалпы ақпарат
Диабеттік нейропатия – қант диабетімен ауыратын адамдарда пайда болатын нервтердің зақымдануы. Бұл жағдай қант диабетінің асқынуы болып табылады.
Себептері
Қант диабеті бар адамдарда қан ағысының әлсіреунен және қанда қант деңгейінің көтерілуінен нерв ұштары зақымдалады. Әдетте бұл ауру қандағы қант деңгейінің бақыланбай көтерілуінен пайда болады.
Шамамен диабетпен ауыратын адамдардың жартысында нерв ұштары зақымдалады. Қант диабеті диагнозы қойылғаннан кейін ауру бірнеше жыл бойы симптомсыз өтеді. Кейбір пациенттерде алғаш рет қант диабеті диагнозы қойылған сәтте нерв ұштарының баяу зақымдалуын байқауға болады.
Симптомдар
Симптомдар негізі баяу және ұзақ жылдары бойы дамиды. Зақымдалған нервке байланысты симптомдар әртүрлі.
Ішек перистальтикасын реттейтін нервтер қазымдалған кезде, сізде ас қорыту кезінде қиындықтар пайда болу мүмкін. Нәтижесінде диабетті қадағалау қиын болады. Ас қорыту қиындауына байланысты симптомдар:
Аз тамақ қабылдаған өзінде, артық тамақтану сезімі.
Қыжыл және желдену
Құсу, іш қату немесе іш өту
Жұтыну кезіндегі қиындықтар
Тамақты ішкеннен бірнеше сағаттан кейін пайда болатын тағам қалдықтарымен құсу
Егер қол мен аяқтағы нервтер зақымдалса, онда тітіркену, күйдіру немесе ауру сезімі пайда болады. Зақымдалу деңгейі үлкейген сайын қолдағы және аяқтағы сезімталдық жоғалады. Сезімталдық жоғалу әсерінен сіз мынадай нәрсені сезбей қалуыңыз мүмкін:
үшкір затты басып кеткенде
сүйел немесе кішкентай кесік пайда болған кезде
қолмен немесе аяқпен қатты ыстық немесе суық сатты тигенде
Егер нәтижесінде жүрек және қан тамырлар нерветір зақымдалса, онда сіз:
Төсектен тез көтерілген кезде (ортостатикалық гипотония) естен тану (обморок)
Жиіліген жүрек ырғағын сезу
Стенокардия немесе жүрек ұстамасы кезіндегі ауру сезімін сезбей қаласыз
Нерв ұштары зақымдалған кездегі басқа симптомдар:
Сексуальды қиындықтар. Ерлерде эрекциямен қиындықтар, ал әйелдерде – қынаптың кеуіп кетуі немесе оргазммен қиындықтар.
Қандағы төмен қант деңгейіне сезімталдықтың жоқтығы.
Қуықпен қиындықтар. Еріксіз зәр шығару немесе қуықты босата алмау.
Тыныштық жағдайда, қалыпты температура кезінде қатты тершеңдік.
Диагностика
Дәрігер тексеру кезінде мынадай ауру белгілерін анықтау мүмкін:
Горизонтальды қалыптан вертикальды қалыпқа тез ауысқан кезде артериальды қысымның төмендеуі
Диагностика кезінде жасалатын зерттеу әдістері:
Электромиография (ЭМГ) – бұлшықеттердің электрлік активтілігін жазу
Нервтік өткізу жылдамдықын тексеру – нервтен өтетін электрлік сигналдарды жазу
Азқасанна аш ішекке тағамның эвакуация жылдамдығын тексеру
Ортостатикалық проба жасау
Емі
Нервтің диабеттік зақымдауын баялау үшін дәрігердің кеңестерін орындаңыз.
Қандағы қант деңгейін оптимальды деңгейді ұстау үшін:
Диета ұстаңыз
Физикалық жаттығуларды күнделікті жасаңыз
Тұрақты түрде қандағы қант деңгейін тексеріп жүріңіз
Қант түсіретін препараттарды немесе инсулинді дәрігердің тағайындауы бойынша қабылдап жүріңіз
Мына симптомдарға байланысты дәрігер сізге ем тағайындайды:
Табанда, аяқа немесе қолдағы ауру сезімі
Құсу, лоқсу немесе тағаммен қорту байланысты басқа қиындықтар
Қуықпен қиындықтар
Эректильды дисфункция немесе қынаптық кебу
Аяқтағы нервтер зақымдалғанда сезімталдық төмендейді. Толық сезімталдықтың жоғалуы пайда болу мүмкін. Нәтижесінде аяқтағы жаралар қиын жазылады. Аяқтарға жасалған дұрыс күтім, осы асқынуды алдын алуға көмектеседі.
Аяқтарға арналған күтім:
Күнделікті аяқты қарау
Дәргерге қаралуға дейін аяқты өзіңіз тексеріңіз.
“Дұрыс” носки және аяқ киімді кию.
Болжамы
Тағайындалған ем ауру сезімін басады және кейбір симптомдарды қадағалауға көмектеседі.
Асқынулар
Зәр шығару жолдарының инфекциясы
Аяқатағы дибеттік ойық жаралар
Стенокардия немесе жүрек ұстамасы кезіндегі ауру сезімін сезбей қалу
Аяқ саусақтарын, табанды немесе тобықты ампутациялау
Дәрігерге қашан қаралу керек?
Диабеттік нейропатия симптомдары пайда болған сәтте дәрігерге хабарласыңыз.
Аударған: Қартанбаев Бақберген Батырбекұлы
Анықтамасы
Себептері
Симптомдары
Емі
Рейе синдромы - 15 жасқа дейінгі балалардың бауырларында май тінінің жиналып қалуы мен мидың ісінуімен жүретін өте сирек кездесетін бұзылыс. Бұл синдром тұмау және желшешек сияқты вирустық инфекцияны басынан өткергеннен кейін болады.Аспирин осы синдромның болуын едәуір арттырады,сондықтан 20 жасқа дейінгі жастарға вирустық инфекция кезінде аспирин қолданбау керек,тек қана дәрігер рұқсатымен ғана қабылдағаны дұрыс.
Рейе синдромының себебі әлі белгісіз,бірақ ол мидағы зат алмасуға қатысатын митохондрий жасушасын вируспен зақымдау арқылы болады деп есептеледі.
Рейе синдромының белгілеріне құсу,ұйқышылдық,есте сақтаудың төмендеуі,әлсіздік,естің адасуы және комаға түсу жатады.
Емі.
Емдеуге арналған нақты хаттамалар жоқ, бірақта антибиотиктерді,инсулинді,кортикостероидтарды,глюкозаны,зәр айдағыш дәрілерді және т.б қолданады.70 % науқастарда жағдайы қалпына келеді, кейбіреулерінде мидың зақымдалуы өмір бойына қалады.
Аударған: Мелис Айбек
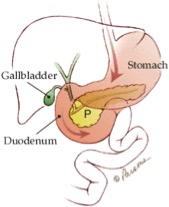
Ұйқы безі – іш қуысында асқазан мен бел омыртқаның арасында орналастын, асқорыту жүйесінің маңызды мүшесі болып табылады. Ол – бауырмен, ішектермен және басқа да ішкі мүшелермен шектеседі. Қалыпты жағдай ұйқы безіның ұзындығы 15 см құрайды. Қалпы – ұзын алмұрт тәрізді. Ұйқы безінің енді бөлігін – басы, ортаңғы бөлігін – денесі, жіңішке бөлігін – құйрығы деп атаайды.
Ұйқы безі –өзінен инсулин және тағы да басқа гормондар бөледі. Бұл гормондар қанағымға еніп, бүкіл организмге таралады. Бұл гормондардың қызметі – тамақ арқылы түскен энергияны сақтау және пайдалану болып табылады. Мысалы, инсулин қандағы қанттың деңгейін қалыпты да ұстап тұруға қатысады. Инсулиннің жеткіліксіздігін – қант диабетті деп атайды.
Ұйқы безі сонымен қатар асты қорытуға қажетті асқорыту сөлін – ферменттерді өндіреді. Өзінен өндірілген асқорыту ферменттері арнайы түтікшелер арқылы он екі ішекке түседі. ( он екі ішек – біз қабылдаған тамақтың алғашқы корытылуы жүретін, аш ішектің бастапқы бөлігі.)
The pancreas is a long flattened gland located deep in the belly (abdomen). Because the pancreas isn’t seen or felt in our day to day lives, most people don't know as much about the pancreas as they do about other parts of their bodies. The pancreas is, however, a vital part of the digestive system and a critical controller of blood sugar levels.
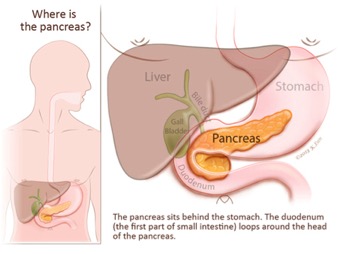
The pancreas is located deep in the abdomen. Part of the pancreas is sandwiched between the stomach and the spine. The other part is nestled in the curve of the duodenum (first part of the small intestine). To visualize the position of the pancreas, try this: touch your right thumb and right "pinkie" fingers together, keeping the other three fingers together and straight. Then, place your hand in the center of your belly just below your lower ribs with your fingers pointing to your left. Your hand will be the approximate shape and at the approximate level of your pancreas.
Because of the deep location of the pancreas, tumors of the pancreas are rarely palpable (able to be felt by pressing on the abdomen). This explains why most symptoms of pancreatic cancer do not appear until the tumor has grown large enough to interfere with the function of the pancreas or other nearby organs such as the stomach, duodenum, liver, or gallbladder.
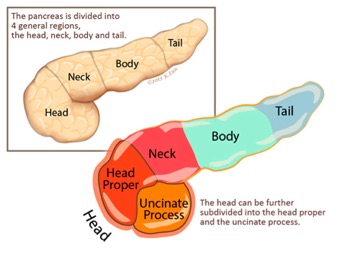
Your doctor may refer to different anatomic parts of the pancreas when discussing your disease. The part of the pancreas that a tumor arises in will affect the symptoms it causes and how it is treated. The pancreas is divided into four main parts.
The head is the widest part of the pancreas. The head of the pancreas is found in the right side of abdomen, nestled in the curve of the duodenum. Using the hand analogy from earlier, the head of the pancreas corresponds to the palm of your hand.
uncinate process
The uncinate is the part of the head of the pancreas that hooks towards the back of the abdomen. The uncinate hooks around two very important blood vessels, the superior mesenteric artery and the superior mesenteric vein. Again, using the hand anaology, the uncinate would correspond to your pinkie and thumb.
neck
The neck is the thin section of the gland between the head and the body of the pancreas. Using the hand analogy, the neck corresponds to your first knuckles.
body
The body is the middle part of the pancreas between the neck and the tail. The superior mesenteric artery and vein run behind this part of the pancreas. Using the hand analogy, the body corresponds to the middle of your fingers.
tail
The tail is the thin tip of the pancreas in the left side of the abdomen, in close proximity with the spleen. Using the hand analogy, the tail corresponds to the tips of your 2nd, 3rd and 4th fingers.
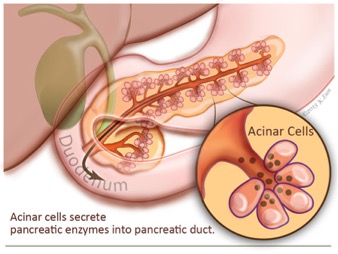
The pancreas is really two glands that are intimately mixed together into one organ. The bulk of the pancreas is composed of “exocrine” cells that produce enzymes to help with the digestion of food. These exocrine cells release their enzymes into a series of progressively larger tubes (called ducts) that eventually join together to form the main pancreatic duct. The main pancreatic duct runs the length of the pancreas and drains the fluid produced by the exocrine cells into the duodenum, the first part of the small bowel.
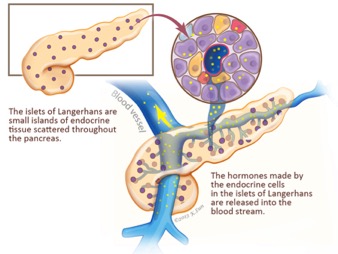
The second functional component of the pancreas is the "endocrine" pancreas. The endocrine pancreas is composed of small islands of cells, called the islets of Langerhans. These endocrine cells don’t release their secretions into the pancreatic ducts, instead they release hormones, such as insulin and glucagon, into the blood stream, and these hormones in turn help control blood sugar (glucose) levels.
Acinar cells
Acinar cells are the exocrine (exo=outward) cells of the pancreas that produce and transport enzymes that are passed into the duodenum where they assist in the digestion of food.
Islets of Langerhans
The islets of Langerhans are the endocrine (endo= within) cells of the pancreas that produce and secrete hormones such as insulin and glucagon into the bloodstream. The pancreatic hormones, insulin and glucagon, work together to maintain the proper level of sugar (glucose) in the blood. Blood sugar is used by the body for energy.
An understanding of the two functional components of the pancreas is important for two reasons.
First, as they grow large tumors of the pancreas will interfere with both of these important bodily functions. When tumors block the exocrine system, patients can develop pancreatitis and pain from the abnormal release of digestive enzymes into the substance of the pancreas instead of into the bowel, and they can develop digestive problems, such as diarrhea, from the incomplete digestion of food. When tumors destroy the endocrine function of the pancreas, patients can develop sugar diabetes (abnormally high blood sugar levels).
The second reason that the two functional components of the pancreas are important to understand is that tumors can arise in either component. The vast majority of tumors of the pancreas arise in the exocrine part and these cancers look like pancreatic ducts under the microscope. These tumors are therefore called "ductal adenocarcinomas," or simply "adenocarcinoma," or even more simply "pancreatic cancer." Less commonly, tumors arise from the endocrine component of the pancreas and these endocrine tumors are called "pancreatic neuroendocrine tumors," or "islet cell tumors" for short.
The pancreas is an integral part of the digestive system, and the flow of the digestive system is often altered during the surgical treatment of pancreatic cancer. Therefore it is helpful to review the normal flow of food and the flow of digestive enzymes of the pancreas before reading about surgical treatment.
Food is carried from the mouth to the stomach by the esophagus. The esophagus is a tube that descends from the mouth down into the abdomen. In the abdomen, the esophagus empties into the stomach where digestive acids made by the stomach break down the food. From the stomach, the partially digested food flows directly into the first part of the small intestine, called the duodenum. It is here in the duodenum that bile from the liver and digestive enzymes from the pancreas enter the digestive system.
The duodenum then leads to the other parts of the small bowel, the jejunum and ileum, where further digestion of food takes place. The ileum then empties into the large bowel (also known as the large intestine), and finally completely digestive material passes out of the body through the anus.
Bile is important to understand because the flow of bile is often blocked by pancreatic cancers, and because the flow of bile is altered during surgery for pancreatic cancer. Bile is a greenish-yellow fluid that aids in the digestion of fats in food. After being produced by cells in the liver, the bile travels down through the bile ducts which merge with the cystic duct from the gallbladder to form the common bile duct. The gallbladder stores extra bile until needed. The common bile duct then passes through the head of the pancreas and joins the pancreatic duct to form the ampulla of Vater which then empties into the duodenum. The flow of bile is indicated by the green arrows.
Understanding that the tube (duct) carrying bile from the liver passes through the pancreas on its way to the intestine, helps us understand why some people with pancreatic cancer develop jaundice (an abnormal yellowing of the skin and eyes). Pancreatic cancers in the head of the pancreas (the bile duct passes through the head of the pancreas) can block the bile duct and in so doing can block the flow of bile out of the liver. The bile backs up and causes jaundice.
Instead of carrying bile, the pancreatic duct carries the fluid containing the digestive enzymes produced by the acinar cells (exocrine cells) of the pancreas. The main pancreatic duct is normally only one-sixteenth of an inch in diameter and it has many small side branches. The main pancreatic duct merges with the bile duct in the head of the pancreas to form the ampulla of Vater (a widening of the duct just before it enters the duodenum). Just as was true for bile, the flow of pancreatic fluid is often blocked by tumors of the pancreas, and altered by pancreatic surgery. The flow of pancreatic fluid is indicated by the dark yellow arrow.
Metabolic syndrome is becoming very common in the United States. Doctors are not sure whether the syndrome is due to one single cause. But many of the risks for the syndrome are related to obesity.
The two most important risk factors for metabolic syndrome are:
· Extra weight around the middle and upper parts of the body (central obesity). This body type may be described as "apple-shaped."
· Insulin resistance. Insulin is a hormone produced in the pancreas. Insulin is needed to help control the amount of sugar in the blood. Insulin resistance means that some cells in the body use insulin less effectively than normal. As a result, blood sugar level rises, which causes insulin to rise. This may increase the amount of body fat.
Other risk factors include:
· Aging
· Genes that make you more likely to develop this condition
· Changes in male, female, and stress hormones
· Lack of exercise
People who have metabolic syndrome often have one or more other factors that may be linked with the condition, including:
· Increased risk for blood clotting
· Increased levels of blood substances that are a sign of inflammation throughout the body
· Small amounts of a protein called albumin in the urine
People with metabolic syndrome have an increased long-term risk of developing heart disease, type 2 diabetes, stroke, kidney disease, and poor blood supply to the legs.
Reye syndrome is sudden (acute) brain damage and liver function problems that do not have a known cause.
This syndrome has occurred in children who were given aspirin when they had chickenpox or the flu. Reye syndrome has become very rare because aspirin is no longer recommended for routine use in children.
Reye syndrome is most often seen in children ages 4 to 12. Most cases that occur with chickenpox are in children ages 5 to 9. Cases that occur with the flu are usually in children ages 10 to 14.
Children with Reye syndrome get sick very suddenly. The syndrome often begins with vomiting, which lasts for many hours. The vomiting is quickly followed by irritable and aggressive behavior. As the condition gets worse, the child may be unable to stay awake and alert.
Unusual placement of arms and legs (decerebrate posture). The arms are extended straight and turned toward the body, the legs are held straight, and the toes are pointed downward
Other symptoms that can occur with this disorder include:
There is no specific treatment for this condition. The health care provider will monitor the pressure in the brain, blood gases, and blood acid-base balance (pH).
Treatments may include:
Breathing support (a breathing machine may be needed during a deep coma)
Never give a child aspirin unless told to do so by your doctor.
When a child must take aspirin, take care to reduce the child's risk of catching a viral illness, such as the flu and chickenpox. Avoid aspirin for several weeks after the child has received a varicella (chickenpox) vaccine.
Note: Other over-the-counter medicines, such as Pepto-Bismol and substances with oil of wintergreen also contain aspirin compounds called salicylates. DO NOT give these to a child who has a cold or fever.