If your child swallowed something that's not sharp or otherwise potentially dangerous and it doesn't seem stuck in his throat, he'll probably do just fine on his own, passing the object in his stool and ending up no worse for the experience.
While you wait, keep a close eye on him and call his doctor if he starts vomiting, drooling, refusing to eat, running a fever, coughing, wheezing, or making a whistling sound when he inhales. Also call the doctor if you don't see the object in your preschooler's stool in the next couple of days. (To check, put the poop in a strainer and run hot water over it.)
If your child may have swallowed something sharp (like a toothpick or needle) or otherwise dangerous (like a watch battery or more than one small magnet), take him to the doctor right away even if he seems fine. These things may need to be removed rather than allowed to pass, because they may perforate your child's esophagus, stomach or intestines; leach dangerous substances; or even create a small electric current.
What will the doctor do?
This will depend on what your child swallowed and whether it seems to be stuck. The doctor may take an X-ray to find out where the object is.
If the doctor thinks that the object will move safely through your child's system on its own (as most objects do), he may tell you to keep an eye on your child and her bowels over the next few days. During this time, he may take additional X-rays to track the progress of the object.
If the object is in your child's airway or stuck in her esophagus or stomach – or if it's dangerous to wait for the object to pass because it's sharp or otherwise hazardous – the doctor will remove it. Most likely he'll use an endoscope (a long, thin, lighted tool) if the object is in her esophagus or stomach. If it's in her airway, he'll use a similar instrument called a bronchoscope. In some instances, surgery is necessary to remove an object.
What if my child is choking on the object?
For information on how to administer first aid for choking, see our guide to choking and CPR. It's a good idea to learn these techniques before you'll ever need them by taking a CPR course.
Is there any way to keep my child from putting stuff in her mouth?
It's very common for a young child to put any old thing in her mouth, but by school age many kids have started to outgrow this method of learning about the world.
If you find that your grade-schooler is still in the habit, you may be able to convince her that it's not such a great idea. Tell her about germs on toys and about how dangerous it can be to swallow something that shouldn't be in her mouth. Then give her gentle reminders as needed.
And again, it's important for you and all of your child's babysitters and childcare providers to be trained in CPR.
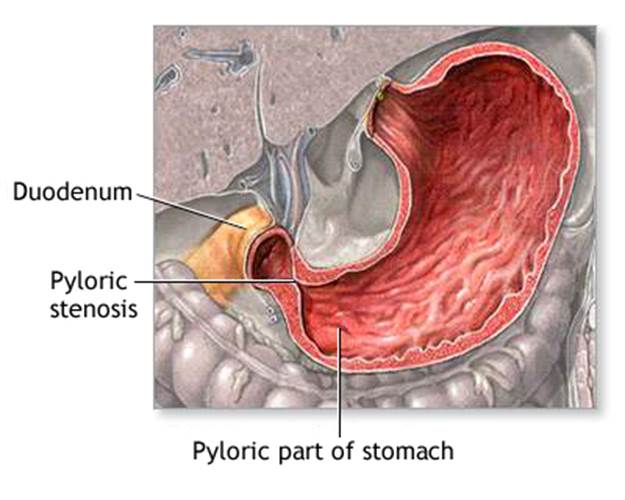
Normally, food passes easily from the stomach into the first part of the small intestine through a valve called the pylorus. With pyloric stenosis, the muscles of the pylorus are thickened. This prevents the stomach from emptying into the small intestine.
The cause of the thickening is unknown. Genes may play a role, since children of parents who had pyloric stenosis are more likely to have this condition.
Pyloric stenosis occurs most often in infants younger than 6 months. It is more common in boys than in girls.
Treatment for pyloric stenosis involves surgery to widen the pylorus. The surgery is called pyloromyotomy.
If putting the infant to sleep for surgery is not safe, a device called an endoscope with a tiny balloon at the end is used. The balloon is inflated to widen the pylorus.
In infants who cannot have surgery, tube feeding or medicine to relax the pylorus is tried.