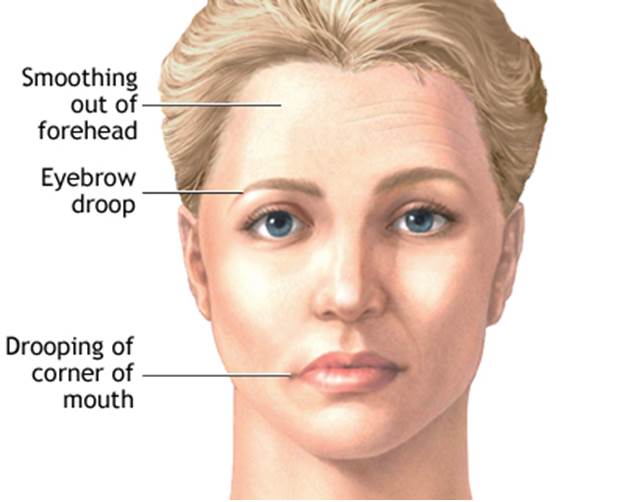
Facial paralysis occurs when a person is no longer able to move some or all of the muscles on one side of the face.
Causes
Facial paralysis is almost always caused by:
Damage or swelling of the facial nerve, which carries signals from the brain to the muscles of the face
Damage to the area of the brain that sends signals to the muscles of the face
In people who are otherwise healthy, facial paralysis is often due to Bell's palsy. This is a condition in which the facial nerve becomes inflamed.
Stroke may cause facial paralysis. With a stroke, other muscles on one side of the body may also be involved.
Facial drooping can be caused by a disorder such as Bell's palsy. This disorder is a mononeuropathy (involvement of a single nerve) that damages the seventh cranial (facial) nerve. The facial nerve controls movement of the muscles of the face.
Facial paralysis that is due to a brain tumor usually develops slowly. Symptoms can include headaches, seizures, or hearing loss.
The doctor may refer you to a physical, speech, or occupational therapist. If facial paralysis from Bell's palsy lasts for more than 6 - 12 months, plastic surgery may be recommended to help the eye close and improve the appearance of the face.
Treatment
Treatment depends on the cause. Follow your health care provider's treatment recommendations.
Home Care
Follow your health care provider's instructions on how to take care of yourself at home. Take any medicines as directed.
If the eye cannot fully close, the cornea must be protected from drying out with prescription eye drops or gel.
When to Contact a Medical Professional
Call your doctor if you have weakness or numbness in your face. Seek emergency medical help right away if you have these symptoms along with a severe headache, seizure, or blindness.
Spinal muscular atrophy (SMA) is a genetic disease that causes muscle weakness and progressive loss of movement.
SMA is caused by deterioration in the nerve cells (motor neurones) connecting the brain and spinal cord to the body's muscles.
As the link between the nerves and muscles breaks down, the muscles used for activities such as crawling, walking, sitting up and moving the head become progressively weaker and shrink (atrophy). Mental abilities are unaffected by SMA.
The term spinal muscular atrophy can be applied to a number of different related conditions.
SMA is classified according to the age symptoms appear and how much physical mobility a person has:
Type I – the most severe type. Symptoms appear in babies less than six months old, and they never develop the ability to sit unsupported.
Type II – less severe than type I. Symptoms usually appear in babies aged 7 to 18 months. Children with Type II can sit unsupported and some are able to stand, but they can't walk independently.
Type III – the mildest type affecting children. Symptoms usually appear after 18 months of age, and children are usually able to reach all the major motor milestones, including independent walking.
Type IV – affects adults.
In the most severe cases (Type I), severe respiratory problems mean children rarely survive beyond two years of age.
Type II SMA may shorten life expectancy, but improvements in care standards mean the majority of people can live long, fulfilling and productive lives. Survival into adulthood is now expected.
Life expectancy is usually unaffected in Types III and IV.
It's not currently possible to treat the underlying genetic fault that causes SMA, although a number of experimental therapies are currently being evaluated in early clinical trials.
However, treatment and support is available to help manage the symptoms and provide people with SMA with the best possible quality of life.
Depending on its severity, treatment may involve:
exercises and equipment to improve mobility and breathing
feeding tubes and nutrition advice
bracing or surgery to treat curvature of the spine (scoliosis)
A range of healthcare professionals are involved in the care of a person with SMA, including:
doctors who specialise in neurology
physiotherapists
occupational therapists
speech and language therapists
if appropriate, respiratory physicians and orthopaedic surgeons
If you have a family history of SMA, you should be able to access genetic testing. This involves checking a sample of your blood for the genetic fault responsible for the condition.
If there's a chance your baby could have SMA, it's also possible to check for this genetic fault during pregnancy, using tests such as chorionic villus sampling (CVS) and amniocentesis. Pre-implantation diagnosis (PGD) is also possible. Families should be referred to a geneticist to discuss all these options.
If a child shows typical signs of SMA, such as obvious muscle weakness, a blood test can usually confirm a diagnosis.
Паралич или слабость мышц на одной стороне лица. Он вызывает свисание одной стороны лица и влияет на вкусовое ощущение, слезообразование и слюнообразование.
В большинстве случаев периферического паралича лицевого нерва нерв, контролирующий мышцы на одной стороне лица, поражен воспалением. Причина этого воспаления не ясна, однако она может быть связана с вирусной инфекцией.
Периферический паралич лицевого нерва наступает неожиданно, часто за ночь, и обычно улучшается или проходит самостоятельно без лечения в течение нескольких недель. Во избежание сухости или травмы можно на ночь наложить повязку на глаз на пораженной стороне. Для уменьшения воспаления врач можетпрописать кортикостероиды.
Что это такое? Бульбоспинальный паралич – это редкое хроническое расстройство, характеризующееся слабостью и возрастающей утомляемостью мышц. Мышечная слабость развивается медленно, в первую очередь, поражая мимические мышцы и, вызывая такие симптомы, как полуопущение век, диплопию, затруднения в речи, в жевании и дыхании.
Точная причина бульбоспинального паралича не известна. Считается, что развитие болезни связано с аутоантителами, направленными против собственной мышечные ткани. Бульбоспинальный паралич может возникнуть в любом возрасте и у женщин, и у мужчин, но наиболее распространен он у молодых женщин, имеющих проблемы с щитовидной железой.
Лечение бульбоспинального паралича включает лекарственные препараты для уменьшения мышечной слабости и их укрепления. В некоторых случаях может помочь удаление щитовидной железы.