Жатыр ішілік ұрықтануға қарсы құрал (ВМС) – Т-тәрізді шағын пластик құрал, жүкті болуға қарсы қолданылатын құрал. Оны жатырдың ішіне орналастырады, ұдайы сонда болады.
Бұл құралды (ВМС) әдетте, дәрігер етеккір кезінде қояды. Оның кез келген түрлерін дәрігер клиникада тез және жеңіл орналастырады.
· дәрігер құрал салынған пластик түтікті іншектің ішіне, одан кейін жатырдың ішіне енгізеді.
· Түтіктегі поршеньнің көмегімен дәрігер құралды жатырдың ішіне енгізеді
· осыдан кейін дәрігер түтікті шығарады, екі шағын қыл жатырдан іншекке қарай шығып тұрады.
Бұл қылдардың әсері:
· дәрігерге немесе әйелге құралдың дұрыс тұруына көз жеткізеді
· керек кезінде құралды жатырдан алып тастауға көмектеседі. Құралды дәрігер ғана алып тасай алады.
Бұл шара өткізілген кезде жайсыздық және ауырсыну болуы мүмкін, бірақ, барлық әйелдерде кездесе бермейді. Құралды алып тастағанда сезілуі мүмкін:
· аздаған ауырсыну және жайсыздық
· түйілу және ауырсыну
· бас айналуы
Кейбір әйелдерде түйілу мен арқасының ауырсынуы құралды алып тастағаннан кейін 1-2 күн бойы сақталуы мүмкін. Кейбірінде бірнеше апта немесе ай бойы созылуы мүмкін. Жайсыздықты жоюға ауырсынуды басатын препараттар көмектеседі.
Сирек болғанымен, құралды қоюдың белгілі бір қауіптері бар:
· құралды қолдануда аздаған жүкті болу қаупі бар. Егер жүктілік пайда болса, дәрігер құралды алып тастайды. Түсік немесе басқа қауіптердің алдын алу үшін.
· Жатырдан тыс жүктіліктің қаупі жоғары, тек жүктілік жатыр ішілік құралды қолдану кезінде пайда болса. Жатырдан тыс жүктілік дегеніміз – жатыр қуысынан басқа жерде пайда болған жүктілік. Бұл жағдай күрделі және өмірге қауіп төндіруі мүмкін.
· сондай –ақ, сирек асқынуы – құралды қою кезінде жатыр қабырғасын зақымдау.
· шара өткізілу кезінде қандай қауіптер болуы мүмкін екендігін
· шара өткізілгеннен кейін нені бақылау қажеттігін
Құралды көбінесе, кез келген уақытта қоюға болады, келесі жағдайлардан басқада:
· босанудан кейін бірден қоюға болмайды
· әдейі немесе кенеттен болған түсіктен кейін бірден қоюға болмайды
Жұқпа кезінде қоюға болмайды.
Құралды енгізу алдында дәрігер ауырсынуды басатын препаратты қабылдауға кеңес беруі мүмкін. Егер іншек немесе жатыр мойны аумағындағы ауырсынуға сезімталдығыңыз бар болса, шараның алдында жергілікті анестезия жасауды сұраңыз.
Шараны өткізгеннен кейін үйге басқа біреуді жеткізіп салуын өтініңіз. Кейбір әйелдерде бірнеше күн бойы әлсіз түйілулер, белдің ауырсынуы және қан бөліністері болады.
Егер прогестероны бар құрал қойылатын болса, ол қойылғаннан кейін 7 күннен кейін әрекет ететін болады. Жыныстық қатынасқа түсу қажеттігі болса, бірінші аптаның ішінде қосымша ұрықтануға қарсы тәсілдерді де қолдану қажет, мысалы, ұрықтануға қарсы таблеткаларды немесе презервативтерді.
Дәрігер құралдың дұрыс орналасқандығына көз жеткізу мақсатында шарадан кейін қайта көрінуді 4-6 аптадан кейінге тағайындайды. Құралдың дұрыс орналасуын қалай тексеру қажеттігін және ол үшін не істеу керектігін дәрігерден сұрап алыңыз.
Құрал толығымен немесе жартылай жатыр қуысынан тыс кетуі мүмкін. Бұлай болғанда шұғыл дәрігерге көрініңіз. Өздігінше жылжып кеткен немесе түскен құралды алуға болмайды.
Келесі симптомдар болса, шүғыл түрде дәрігерге көрініңіз:
Материалды дайындаған Алмаз Шарман, медицина профессоры.
Аударған: Асель Стамбекова.
Редакциялаған: Александр Корольков.
The uterus is a hollow muscular organ located in the female pelvis between the bladder and rectum. The ovaries produce the eggs that travel through the fallopian tubes. Once the egg has left the ovary it can be fertilized and implant itself in the lining of the uterus. The main function of the uterus is to nourish the developing fetus prior to birth.
Scarring from sexually transmitted infections, injury, or surgery
Smoking
Toxins in the environment
Vasectomy or failure of vasectomy reversal
Healthy couples under age 30 who have sex regularly will have a 25% to 30% per month chance of getting pregnant each month.
A woman is most fertile in her early 20s. The chance a woman can get pregnant drops greatly after age 35 (and especially after age 40). The age when fertility starts to decline varies from woman to woman.
Infertility problems and miscarriage rates increase significantly after 35 year of age. There are now options for early egg retrieval and storage for women in their 20's. This will help ensure a successful pregnancy if childbearing is delayed until after age 35. This is an expensive option, but for women who know they will need to delay childbearing, it may be worth considering.
Exams and Tests
Deciding when to get treated for infertility depends on your age. Health care providers often suggest that women under 30 try to get pregnant on their own for 1 year before getting tested.
Many experts recommend that women over 35 attempt conception for only 6 months. If a pregnancy does not occur within that time, they should talk to their provider.
Infertility testing involves a medical history and physical exam for both partners.
Blood and imaging tests are most often needed. In women, these may include:
Blood tests to check hormone levels, including progesterone and follicle stimulating hormone (FSH)
Home urine ovulation detection kits
Measurement of body temperature every morning to see if the ovaries are releasing eggs
Treatment depends on the cause of infertility. It may involve:
Education and counseling about the condition
Fertility treatments such as intrauterine insemination (IUI) and in vitro fertilization (IVF)
Medicines to treat infections and clotting disorders
Medicines that help the growth and release of eggs from the ovaries
Couples can increase the chances of becoming pregnant each month by having sex at least every 3 days before and during ovulation.
Ovulation occurs about 2 weeks before the next menstrual cycle (period) starts. Therefore, if a woman gets her period every 28 days the couple should have sex at least every 3 days between the 10th and 18th day after her period starts.
Having sex before ovulation occurs is especially helpful.
Sperm can live inside a woman's body for at least 3 days.
However, a woman's egg can only be fertilized by the sperm for a few hours after it is released.
Women who are under or overweight may increase their chances of becoming pregnant by getting to a healthier weight.
Support Groups
Many people find it helpful to take part in support groups for people with similar concerns. You can ask your provider to recommend local groups.
Outlook (Prognosis)
As many as 1 in 5 couples diagnosed with infertility eventually become pregnant without treatment.
More than half of couples with infertility become pregnant after treatment. This figure does not include advanced techniques such as in vitro fertilization (IVF).
When to Contact a Medical Professional
Call your provider if you are unable to get pregnant.
Prevention
Preventing sexually transmitted infections (STIs), such as gonorrhea and chlamydia, may reduce your risk of infertility.
Maintaining a healthy diet, weight, and lifestyle may increase your chance of getting pregnant and having a healthy pregnancy.
Uterine fibroids are tumors that grow in a woman's womb (uterus). These growths are not cancer (benign).
Uterine diseases The uterus, or womb, is the place where a baby grows when a woman is pregnant. The first sign of a problem with the uterus may be bleeding between periods or after sex. Causes can include hormones, thyroid problems, fibroids, polyps, cancer, infection, or pregnancy.
Treatment depends on the cause. Sometimes birth control pills treat hormonal imbalances. If a thyroid problem is the cause, treating it may also stop the bleeding. If you have cancer or hyperplasia, an overgrowth of normal cells in the uterus, you may need surgery.
With two other uterine problems, tissue that normally lines the uterus grows where it is not supposed to. In endometriosis, it grows outside the uterus. In adenomyosis, it grows in the uterus's outside walls. Pain medicine may help. Other treatments include hormones and surgery.
Uterine fibroids are common. As many as 1 in 5 women may have fibroids during their childbearing years. Half of all women have fibroids by age 50.
Fibroids are rare in women under age 20. They are more common in African-Americans than Caucasians.
No one knows exactly what causes fibroids. They are thought to be caused by:
Hormones in the body
Genes (may run in families)
Fibroids can be so tiny that you need a microscope to see them. They can also grow very large. They may fill the entire uterus and may weigh several pounds. Although it is possible for just one fibroid to develop, usually there are more than one.
Fibroids can grow:
In the muscle wall of the uterus (myometrial)
Just under the surface of the uterine lining (submucosal)
Just under the outside lining of the uterus (subserosal)
On a long stalk on the outside the uterus or inside the uterus (pedunculated)
Heavy bleeding during your period, sometimes with blood clots
Periods that may last longer than normal
Needing to urinate more often
Pelvic cramping or pain with periods
Feeling fullness or pressure in your lower belly
Pain during intercourse
Often, you can have fibroids and not have any symptoms. Your health care provider may find them during a physical exam or other test. Fibroids often shrink and cause no symptoms in women who have gone through menopause. A recent study also showed that some small fibroids shrink in premenopausal women.
Treatment for the symptoms of fibroids may include:
Birth control pills to help control heavy periods
Intrauterine devices (IUDs) that release hormones to help reduce heavy bleeding and pain
Iron supplements to prevent or treat anemia due to heavy periods
Pain relievers such as ibuprofen or naprosyn for cramps or pain
Hormone therapy shots to help shrink fibroids (done only for a short time)
Watchful waiting: You may have pelvic exams or ultrasounds every once in a while to check the fibroid's growth
Surgery and procedures used to treat fibroids include:
Hysteroscopy. This procedure can remove fibroids growing inside the uterus.
Uterine artery embolization.This procedure stops the blood supply to the fibroid, causing it to shrink and die. This may be a good option if you want to have children in the future.
Myomectomy. This surgery removes the fibroids from the uterus. This also may be a good choice if you want to have children. It won't prevent fibroids from growing again.
Hysterectomy. This surgery removes the uterus completely. It may be an option if you don't want children, medicines do not work, and you cannot have any other procedures.
If you have fibroids without symptoms, you may not need treatment.
If you have fibroids, they may grow if you become pregnant. This is due to the increased blood flow and higher estrogen levels. The fibroids usually return to their original size after your baby is born.
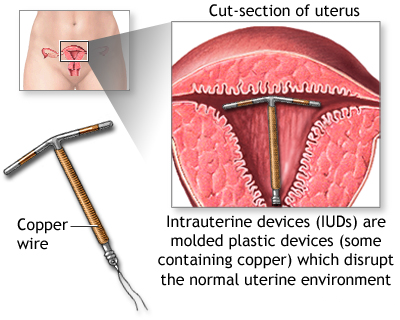
An intrauterine device (IUD) is a small plastic T-shaped device used for birth control. It is inserted into the uterus where it stays to prevent pregnancy.
An IUD is usually inserted by your health care provider during your monthly period. Either type can be inserted quickly and easily in the provider's office or clinic.
The provider slides a plastic tube containing the IUD through the vagina and into the uterus.
Using a plunger in the tube, the provider pushes the IUD into the uterus.
The provider removes the tube, leaving two small strings that dangle outside the cervix within the vagina.
The strings have two purposes:
They let the provider or woman check that the IUD stays properly in position.
They are used to pull the IUD out of the uterus when it is time to remove it. This should only be done by a health care provider.
This procedure can cause discomfort and pain, but not all women have the same side effects. During insertion, you may feel:
Little pain and some discomfort
Cramping and pain
Dizzy or light-headed
Some women have cramps and backaches for 1 to 2 days after insertion. Other may have cramps and backaches for weeks or months. Over-the-counter pain relievers can ease the discomfort.
There is a small chance of getting pregnant while using an IUD. If you do get pregnant, your provider can remove the IUD to lower the risk of miscarriage or other problems.
A higher risk of an ectopic pregnancy, but only if you do get pregnant while using an IUD. An ectopic pregnancy is one that occurs outside the womb. It can be serious, even life-threatening.
A rare chance the IUD may make a hole in the uterine wall when it is inserted.
Talk with your provider about whether an IUD is a good choice for you.
Also ask your provider:
What you can expect during the procedure
What your risks might be
What you should watch for after the procedure
For the most part, an IUD can be inserted at any time:
Right after giving birth
After an elective or spontaneous miscarriage
If you have an infection, you should NOT have an IUD inserted.
Your provider may advise you to take an over-the-counter painkiller before getting the IUD inserted. If you are sensitive to pain in your vagina or cervix, ask for a local anesthetic to be applied before the procedure starts.
You may want to have someone drive you home after the procedure. Some women have mild cramping, low backache, and spotting for a couple of days.
If you have a progestin-releasing IUD, it takes about 7 days for it to start to work. You do not need to wait to have sex. But you should use a backup form of birth control, such as a condom, for the first week.
Your provider will want to see you 4 to 6 weeks after the procedure to be sure the IUD is still in place. Ask your provider to show you how to check that the IUD is still in place, and how often you should check it.
An IUD can slip partly or all of the way out of your uterus. If this happens, contact your health care provider right away. Do NOT try to remove an IUD that has come part of the way out or has slipped out of place.
Call your health care provider right away if you have:
Внутриматочное средство (ВМС) представляет собой небольшое пластиковое Т-образное устройство, используемое для контроля рождаемости. Оно устанавливается в полости матки, где в последующем и остается, с целью предотвращения беременности.
ВМС обычно устанавливается врачом во время менструации. Любой тип ВМС может быть быстро и легко установлен в клинике на приеме у врача.
· Врач вводит пластиковую трубку, содержащую ВМС в полость влагалища, а затем в матку.
· При помощи поршня, расположенного в трубке, врач вводит ВМС в полость матки
· После этого врач выводит трубку, оставляя две маленькие струны, которые свисают из матки в полость влагалища
У данных струн имеется два назначения:
· Они помогают врачу или самой женщине убедиться в том, что ВМС находится в правильном положении
· Они позволяют извлечь ВМС из полости матки, когда это необходимо. Извлечение ВМС проводится только врачом.
При проведении данной процедуры могут возникнуть дискомфорт и боль, но данный побочный эффект встречается не у всех женщин. При извлечении ВМС вы можете чувствовать:
· Небольшую боль и дискомфорт
· Спазмы и боль
· Головокружение
У некоторых женщин спазмы и боль в спине могут сохраняться в течение 1-2 дней после удаления ВМС. У некоторых данные симптомы могут длиться в течение нескольких недель или месяцев. Облегчить дискомфорт могут помочь обезболивающие препараты.
· Это длительный и эффективный метод контроля рождаемости
· Отсутствуют риски и побочные эффекты, характерные для приема контрацептивных гормонов
Но перед тем, как установить ВМС, вам необходимо больше узнать о том, что это такое.
ВМС позволяет предотвратить беременность в течение 3-10 лет. Длительность данной способности зависит от того, какой тип ВМС используется.
ВМС также может быть использовано в качестве экстренного метода контрацепции. ВМС может быть установлено в течение 5 дней после незащищенного полового акта.
Хотя это и возникает редко, установка ВМС может быть сопряжена с определенными рисками:
· При использовании ВМС существует небольшой риск забеременеть. Если наступила беременность, врач может извлечь ВМС. Чтобы снизить риск возникновения выкидыша и других проблем.
· Более высок риск внематочной беременности, но только при условии, что беременность наступила при использовании ВМС. Внематочной называют беременность, которая возникла вне полости матки. Данное состояние может быть серьезным, даже жизнеугрожающим.
· Также редким осложнением является перфорирование стенки матки при установке ВМС.
· За чем вы должны наблюдать после проведения процедуры
В большинстве случаем ВМС можно ввести в любой момент:
· Сразу после родов
· После намеренного или спонтанного аборта
Если у вас инфекция, вам не следует устанавливать ВМС.
Перед введением ВМС врач может посоветовать вам принять обезболивающий препарат. Если вы чувствительны к боли в области влагалища и шейки матки, попросите провести местную анестезию перед началом проведения процедуры.
После проведения процедуры вам лучше попросить кого-либо отвезти вас домой. У некоторых женщин могут быть неинтенсивные спазмы, боль в области поясницы и кровянистые выделения в течение нескольких дней.
Если вам устанавливается ВМС с прогестероном, оно начинает функционировать через 7 дней после установки. Вам нет необходимости ждать, чтобы заниматься сексом. Но для этого в течение первой недели вам необходимо воспользоваться резервными методами контрацепции, такими как противозачаточные таблетки или презервативы.
Врач может назначить вам повторный прием через 4-6 недель после процедуры. Чтобы убедиться, что ВМС располагается правильно. Попросите врача научить вас, как проверять правильно ли располагается ВМС, и как часто вам следует это делать.
ВМС может полностью или частично находиться вне полости матки. Если это произошло, незамедлительно обратитесь к врачу. Не пытайтесь самостоятельно переместить сместившееся или выпавшее ВМС.
Незамедлительно обратитесь к врачу при наличии следующих симптомов:
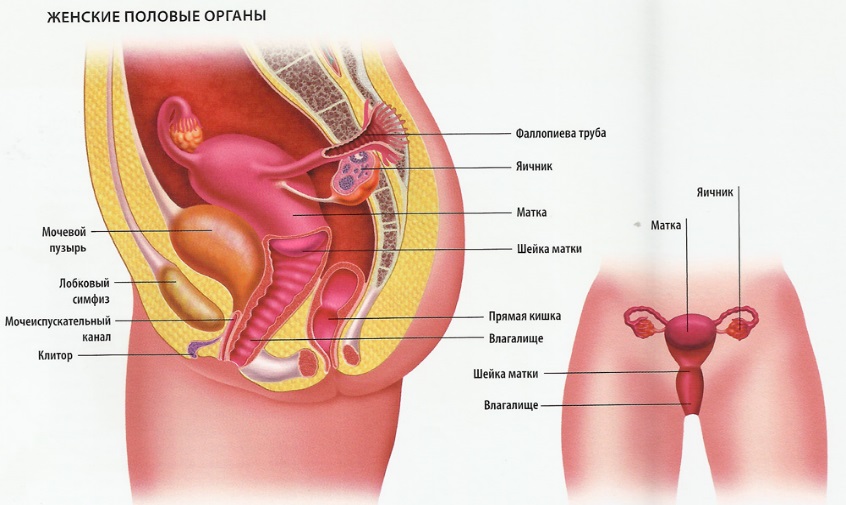
Матка является частью репродуктивной системы женщины. Она представляет собой полый орган грушевидной формы, в котором происходит развитие плода. Матка расположена в малом тазу между мочевым пузырем и прямой кишкой. Матка имеет шейку, которая представляет собой сужение, расположенной в нижней части матки. Широкая часть матки, расположенная выше шейки, называется телом матки. Куполообразная верхняя часть органа называется дном матки. Фаллопиевы трубы представляют собой отростки матки, расположенные по обе стороны органа. Они заканчиваются яичниками.
Стенка матки состоит из двух слоев. Внутренний слой называется эндометрием. Наружный слой стенки матки представлен мышечной тканью и называется миометрием.
У женщин детородного возраста каждый месяц происходит утолщение эндометрия, что связано с подготовкой матки к беременности. Если беременность не наступает, толстый внешний слой эндометрия отторгается и выходит через влагалище вместе с кровяными массами. Это явление называется менструацией.
Фиброма матки – это доброкачественные наросты в матке. Фибромы могут образоваться внутри матки, в пределах мышечных стенок матки, либо с её наружной стороны.
У многих женщин с фибромой матки симптомы не проявляются. Если симптомы имеются, то они обычно слабые и могут включать:
Аномальное влагалищное кровотечение, такое как более сильные, продолжительные периоды или кровотечения между периодами.
Тазовая боль, включая боль во время секса.
Непроходящая боль в пояснице.
Проблемы мочеиспускания.
Иногда фиброма матки может вызвать более серьезные проблемы, например, бесплодие, закупорку мочевыводящего тракта или кишки, или анемию.
Домашнее лечение обычно смягчает симптомы и сдерживает слабые симптомы фибромы матки. В некоторых случаях, например, при появлении более серьезных симптомов или других осложнений, может потребоваться медикаментозное лечение или операция.
Что это такое?Бесплодие определяется как неспособность пары забеременеть после 2 лет половой жизни без использования противозачаточных средств. Приблизительно 80 процентов женщин фертильного возраста способны зачать ребенка. Однако каждая восьмая супружеская пара бесплодна.
Каковы причины? Бесплодие может быть вызвано проблемами как мужчины, так и женщины. Распространенные причины бесплодия – проблемы с овуляцией и выработкой спермы, заболевания фаллопиевых труб, матки и простаты, неправильный график ведения половой жизни. В некоторых случаях причина не может быть выявлена (необъяснимое бесплодие).


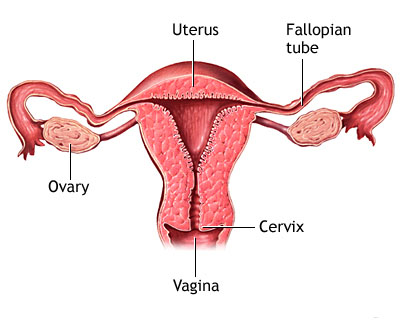
 Матка имеет шейку, которая представляет собой сужение, расположенной в нижней части матки. Широкая часть матки, расположенная выше шейки, называется телом матки. Куполообразная верхняя часть органа называется дном матки. Фаллопиевы трубы представляют собой отростки матки, расположенные по обе стороны органа. Они заканчиваются яичниками.
Матка имеет шейку, которая представляет собой сужение, расположенной в нижней части матки. Широкая часть матки, расположенная выше шейки, называется телом матки. Куполообразная верхняя часть органа называется дном матки. Фаллопиевы трубы представляют собой отростки матки, расположенные по обе стороны органа. Они заканчиваются яичниками.