Ученые из Массачусетского технологического института в США совместно со специалистами из Гарвардской медицинской школы и университета Висконсина обнаружили химические соединения, которые позволяют клеткам печени воспроизводиться в лабораторных условиях.
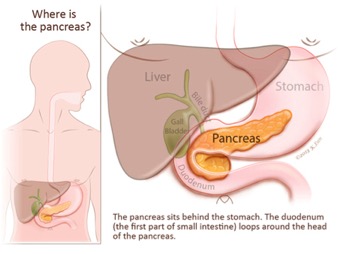
The pancreas is a long flattened gland located deep in the belly (abdomen). Because the pancreas isn’t seen or felt in our day to day lives, most people don't know as much about the pancreas as they do about other parts of their bodies. The pancreas is, however, a vital part of the digestive system and a critical controller of blood sugar levels.
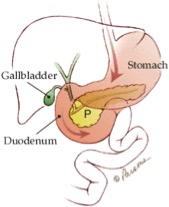
The pancreas is located deep in the abdomen. Part of the pancreas is sandwiched between the stomach and the spine. The other part is nestled in the curve of the duodenum (first part of the small intestine). To visualize the position of the pancreas, try this: touch your right thumb and right "pinkie" fingers together, keeping the other three fingers together and straight. Then, place your hand in the center of your belly just below your lower ribs with your fingers pointing to your left. Your hand will be the approximate shape and at the approximate level of your pancreas.
Because of the deep location of the pancreas, tumors of the pancreas are rarely palpable (able to be felt by pressing on the abdomen). This explains why most symptoms of pancreatic cancer do not appear until the tumor has grown large enough to interfere with the function of the pancreas or other nearby organs such as the stomach, duodenum, liver, or gallbladder.
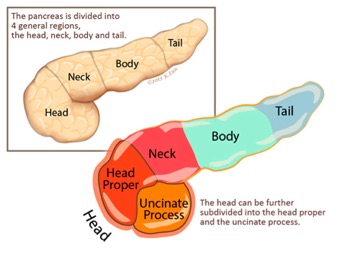
Your doctor may refer to different anatomic parts of the pancreas when discussing your disease. The part of the pancreas that a tumor arises in will affect the symptoms it causes and how it is treated. The pancreas is divided into four main parts.
The head is the widest part of the pancreas. The head of the pancreas is found in the right side of abdomen, nestled in the curve of the duodenum. Using the hand analogy from earlier, the head of the pancreas corresponds to the palm of your hand.
uncinate process
The uncinate is the part of the head of the pancreas that hooks towards the back of the abdomen. The uncinate hooks around two very important blood vessels, the superior mesenteric artery and the superior mesenteric vein. Again, using the hand anaology, the uncinate would correspond to your pinkie and thumb.
neck
The neck is the thin section of the gland between the head and the body of the pancreas. Using the hand analogy, the neck corresponds to your first knuckles.
body
The body is the middle part of the pancreas between the neck and the tail. The superior mesenteric artery and vein run behind this part of the pancreas. Using the hand analogy, the body corresponds to the middle of your fingers.
tail
The tail is the thin tip of the pancreas in the left side of the abdomen, in close proximity with the spleen. Using the hand analogy, the tail corresponds to the tips of your 2nd, 3rd and 4th fingers.
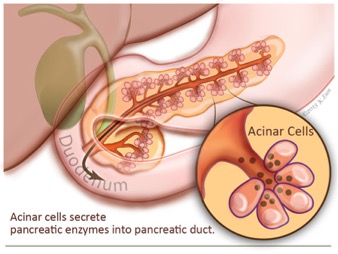
The pancreas is really two glands that are intimately mixed together into one organ. The bulk of the pancreas is composed of “exocrine” cells that produce enzymes to help with the digestion of food. These exocrine cells release their enzymes into a series of progressively larger tubes (called ducts) that eventually join together to form the main pancreatic duct. The main pancreatic duct runs the length of the pancreas and drains the fluid produced by the exocrine cells into the duodenum, the first part of the small bowel.
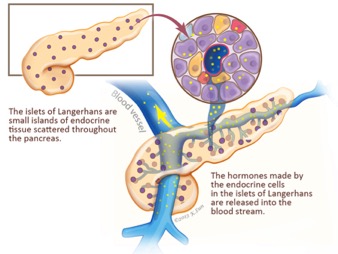
The second functional component of the pancreas is the "endocrine" pancreas. The endocrine pancreas is composed of small islands of cells, called the islets of Langerhans. These endocrine cells don’t release their secretions into the pancreatic ducts, instead they release hormones, such as insulin and glucagon, into the blood stream, and these hormones in turn help control blood sugar (glucose) levels.
Acinar cells
Acinar cells are the exocrine (exo=outward) cells of the pancreas that produce and transport enzymes that are passed into the duodenum where they assist in the digestion of food.
Islets of Langerhans
The islets of Langerhans are the endocrine (endo= within) cells of the pancreas that produce and secrete hormones such as insulin and glucagon into the bloodstream. The pancreatic hormones, insulin and glucagon, work together to maintain the proper level of sugar (glucose) in the blood. Blood sugar is used by the body for energy.
An understanding of the two functional components of the pancreas is important for two reasons.
First, as they grow large tumors of the pancreas will interfere with both of these important bodily functions. When tumors block the exocrine system, patients can develop pancreatitis and pain from the abnormal release of digestive enzymes into the substance of the pancreas instead of into the bowel, and they can develop digestive problems, such as diarrhea, from the incomplete digestion of food. When tumors destroy the endocrine function of the pancreas, patients can develop sugar diabetes (abnormally high blood sugar levels).
The second reason that the two functional components of the pancreas are important to understand is that tumors can arise in either component. The vast majority of tumors of the pancreas arise in the exocrine part and these cancers look like pancreatic ducts under the microscope. These tumors are therefore called "ductal adenocarcinomas," or simply "adenocarcinoma," or even more simply "pancreatic cancer." Less commonly, tumors arise from the endocrine component of the pancreas and these endocrine tumors are called "pancreatic neuroendocrine tumors," or "islet cell tumors" for short.
The pancreas is an integral part of the digestive system, and the flow of the digestive system is often altered during the surgical treatment of pancreatic cancer. Therefore it is helpful to review the normal flow of food and the flow of digestive enzymes of the pancreas before reading about surgical treatment.
Food is carried from the mouth to the stomach by the esophagus. The esophagus is a tube that descends from the mouth down into the abdomen. In the abdomen, the esophagus empties into the stomach where digestive acids made by the stomach break down the food. From the stomach, the partially digested food flows directly into the first part of the small intestine, called the duodenum. It is here in the duodenum that bile from the liver and digestive enzymes from the pancreas enter the digestive system.
The duodenum then leads to the other parts of the small bowel, the jejunum and ileum, where further digestion of food takes place. The ileum then empties into the large bowel (also known as the large intestine), and finally completely digestive material passes out of the body through the anus.
Bile is important to understand because the flow of bile is often blocked by pancreatic cancers, and because the flow of bile is altered during surgery for pancreatic cancer. Bile is a greenish-yellow fluid that aids in the digestion of fats in food. After being produced by cells in the liver, the bile travels down through the bile ducts which merge with the cystic duct from the gallbladder to form the common bile duct. The gallbladder stores extra bile until needed. The common bile duct then passes through the head of the pancreas and joins the pancreatic duct to form the ampulla of Vater which then empties into the duodenum. The flow of bile is indicated by the green arrows.
Understanding that the tube (duct) carrying bile from the liver passes through the pancreas on its way to the intestine, helps us understand why some people with pancreatic cancer develop jaundice (an abnormal yellowing of the skin and eyes). Pancreatic cancers in the head of the pancreas (the bile duct passes through the head of the pancreas) can block the bile duct and in so doing can block the flow of bile out of the liver. The bile backs up and causes jaundice.
Instead of carrying bile, the pancreatic duct carries the fluid containing the digestive enzymes produced by the acinar cells (exocrine cells) of the pancreas. The main pancreatic duct is normally only one-sixteenth of an inch in diameter and it has many small side branches. The main pancreatic duct merges with the bile duct in the head of the pancreas to form the ampulla of Vater (a widening of the duct just before it enters the duodenum). Just as was true for bile, the flow of pancreatic fluid is often blocked by tumors of the pancreas, and altered by pancreatic surgery. The flow of pancreatic fluid is indicated by the dark yellow arrow.
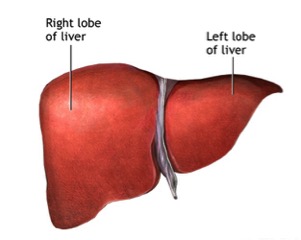
Your liver is the largest organ inside your body. It helps your body digest food, store energy, and remove poisons.
There are many kinds of liver diseases. Viruses cause some of them, like hepatitis A, hepatitis B, and hepatitis C. Others can be the result of drugs, poisons or drinking too much alcohol. If the liver forms scar tissue because of an illness, it's called cirrhosis. Jaundice, or yellowing of the skin, can be one sign of liver disease.
Newborn jaundice is when a baby has high levels of bilirubin in the blood. Bilirubin is a yellow substance that the body creates when it replaces old red blood cells. The liver helps break down the substance so it can be removed from the body in the stool.
High levels of bilirubin makes your baby's skin and whites of the eyes look yellow. This is called jaundice.
Newborn jaundice (producing yellow skin) can have many causes, but the majority of these infants have a condition called physiological jaundice, a natural occurrence in the newborn due to the immature liver. This type of jaundice is short term, generally lasting only a few days. Jaundice should be evaluated by a physician until decreasing or normal levels of bilirubin are measured in the blood.
It is normal for a baby's bilirubin level to be a bit higher after birth.
When the baby is growing in the mother's womb, the placenta removes bilirubin from the baby's body. The placenta is the organ that grows during pregnancy to feed the baby. After birth, the baby's liver starts doing this job. This can take a while.
Most newborns have some yellowing of the skin, or jaundice. This is called "physiological jaundice." It is harmless, and usually is worst when the baby is 2 - 4 days old. It goes away within 2 weeks and doesn't usually cause a problem.
Two types of jaundice may occur in newborns who are breast fed. Both types are usually harmless.
Breastfeeding jaundice is seen in breastfed babies during the first week of life, especially in babies who do not nurse well or if the mother's milk is slow to come in.
Breast milk jaundice may appear in some healthy, breastfed babies after day 7 of life. It usually peaks during weeks 2 and 3. It may last at low levels for a month or more. It may be due to how substances in the breast milk affect how bilirubin breaks down in the liver. Breast milk jaundice is different than breastfeeding jaundice.
Severe newborn jaundice may occur if your baby has a condition that increases the number of red blood cells that need to be replaced in the body, such as:
Abnormal blood cell shapes
Blood type mismatch between the mother and the baby
Bleeding underneath the scalp (cephalohematoma) caused by a difficult delivery
Higher levels of red blood cells, which is more common in small-for-gestational-age babies and some twins
Infection
Lack (deficiency) of certain important proteins, called enzymes
Things that make it harder for the baby's body to remove bilirubin may also lead to more severe jaundice, including:
Certain medications
Congenital infections, such as rubella, syphilis, and others
Diseases that affect the liver or biliary tract, such as cystic fibrosis or hepatitis
Low oxygen level (hypoxia)
Infections (such as sepsis)
Many different genetic or inherited disorders
Babies who are born too early (premature) are more likely to develop jaundice than full-term babies.
Jaundice causes a yellow color of the skin. The color sometimes begins on the face and then moves down to the chest, belly area, legs, and soles of the feet.
Sometimes, infants with significant jaundice have extreme tiredness and poor feeding.
Doctors, nurses, and family members will watch for signs of jaundice at the hospital, and after the newborn goes home.
Any infant who appears jaundiced should have bilirubin levels measured right away. This can be done with a blood test.
Many hospitals check total bilirubin levels on all babies at about 24 hours of age. Hospitals use probes that can estimate the bilirubin level just by touching the skin. High readings need to be confirmed with blood tests.
Tests that will likely be done include:
Complete blood count
Coomb's test
Reticulocyte count
Further testing may be needed for babies who need treatment or whose total bilirubin levels are rising more quickly than expected.
When determining treatment, the doctor must consider:
The baby's bilirubin level
How fast the level has been rising
Whether the baby was born early (babies born early are more likely to be treated at lower bilirubin levels)
How old the baby is now
Your child will need treatment if the bilirubin level is too high or is rising too quickly.
Keep the baby well hydrated with breast milk or formula. Frequent feedings (up to 12 times a day) encourage frequent bowel movements, which help remove bilirubin through the stools. Ask your doctor before giving your newborn extra formula.
Some newborns need to be treated before they leave the hospital. Others may need to go back to the hospital when they are a few days old. Treatment in the hospital usually lasts 1 to 2 days.
Sometimes special blue lights are used on infants whose levels are very high. This is called phototherapy. These lights work by helping to break down bilirubin in the skin.
The infant is placed under artificial light in a warm, enclosed bed to maintain constant temperature. The baby will wear only a diaper and special eye shades to protect the eyes. The American Academy of Pediatrics recommends that breastfeeding be continued through phototherapy, if possible. Rarely, the baby may have an intravenous (IV) line to deliver fluids.
If the bilirubin level is not too high or is not rising quickly, you can do phototherapy at home with a fiberoptic blanket, which has tiny bright lights in it. You may also use a bed that shines light up from the mattress.
You must keep the light therapy on your child's skin and feed your child every 2 to 3 hours (10 to 12 times a day).
A nurse will come to your home to teach you how to use the blanket or bed, and to check on your child.
The nurse will return daily to check your child's weight, feedings, skin, and bilirubin levels.
You will be asked to count the number of wet and dirty diapers.
In the most severe cases of jaundice, an exchange transfusion is required. In this procedure, the baby's blood is replaced with fresh blood. Treating severely jaundiced babies with intravenous immunoglobulin may also be very effective at reducing bilirubin levels.
Usually newborn jaundice is not harmful. For most babies, jaundice usually gets better without treatment within 1 to 2 weeks.
Very high levels of bilirubin can damage the brain. This is called kernicterus. However, the condition is almost always diagnosed before levels become high enough to cause this damage.
For babies who need treatment, the treatment is usually effective.
In newborns, some degree of jaundice is normal and probably not preventable. The risk of significant jaundice can often be reduced by feeding babies at least 8 to 12 times a day for the first several days and by carefully identifying infants at highest risk.
All pregnant women should be tested for blood type and unusual antibodies. If the mother is Rh negative, follow-up testing on the infant's cord is recommended. This may also be done if the mother's blood type is O+, but it is not needed if careful monitoring takes place.
Careful monitoring of all babies during the first 5 days of life can prevent most complications of jaundice. Ideally, this includes:
Considering a baby's risk for jaundice
Checking bilirubin level in the first day or so
Scheduling at least one follow-up visit the first week of life for babies sent home from the hospital in 72 hours
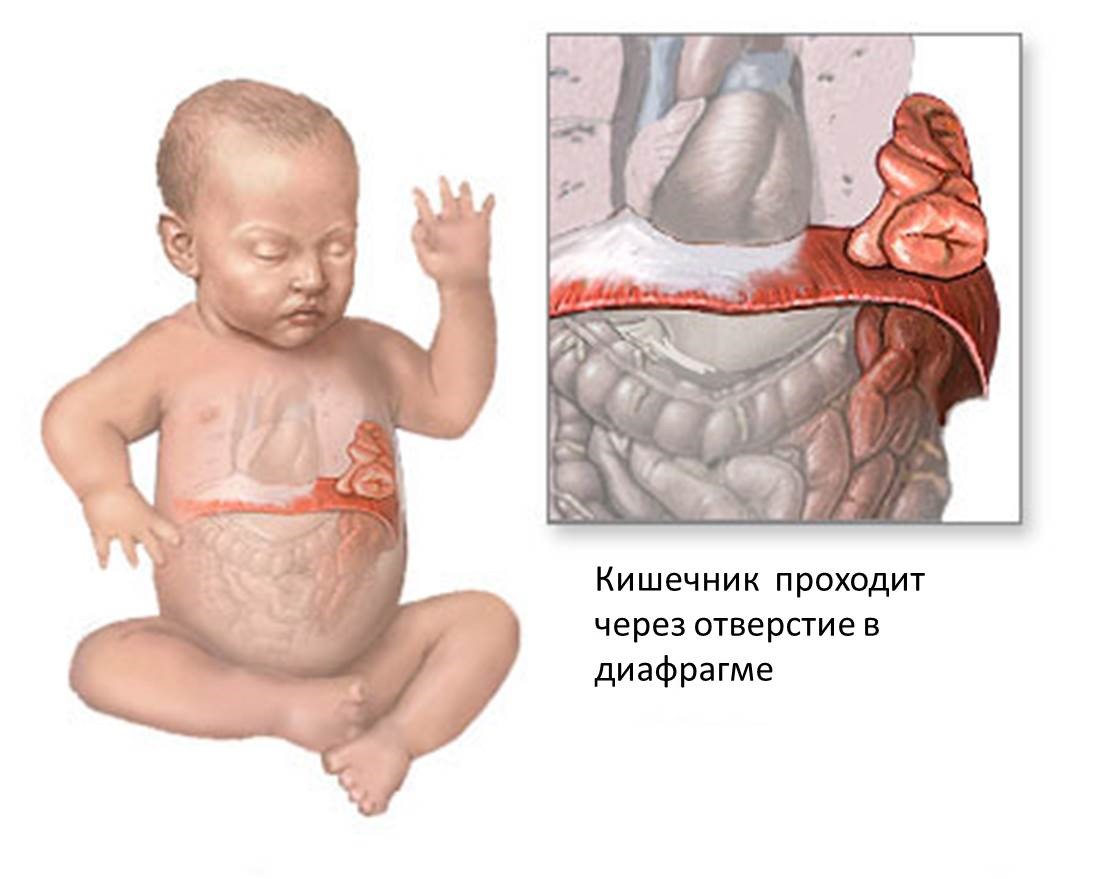
A diaphragmatic hernia is a birth defect in which there is an abnormal opening in the diaphragm, the muscle that helps you breathe. The opening allows part of the organs from the belly (stomach, spleen, liver, and intestines) to go up into the chest cavity near the lungs.
An abnormal opening in the diaphragm that allows part of the abdominal organs to migrate into the chest cavity, occurring before birth.
Causes
A diaphragmatic hernia is caused by the improper joining of structures during fetal development. As a result, the abdominal organs such as the stomach, small intestine, spleen, part of the liver, and the kidney appear in the chest cavity. The lung tissue on the affected side is thus not allowed to completely develop.
Congenital diaphragmatic hernia is seen in 1 out of every 2,200 to 5,000 live births. Most affect the left side. Having a parent or sibling with the condition slightly increases your risk.
Symptoms
Severe breathing difficulty almost always develops shortly after the baby is born, because of ineffective movement of the diaphragm and crowding of the lung tissue, which causes collapse.
Abdomen feels less full on examination by touch (palpation)
A chest x-ray may show abdominal organs in chest cavity.
Treatment
A diaphragmatic hernia is an emergency that requires surgery. Surgery is done to place the abdominal organs into the proper position and repair the opening in the diaphragm.
The infant will need breathing support until he or she recovers from surgery. Some infants are placed on a heart/lung bypass machine, which gives the lungs a chance to recover and expand after surgery.
If a diaphragmatic hernia is diagnosed during pregnancy (around 24 to 28 weeks), fetal surgery may be considered.
Outlook (Prognosis)
The outcome of surgery depends on how well the baby's lungs have developed and also on whether there are any other congenital problems. Usually the outlook is very good for infants who have enough lung tissue and have no other problems.
With advances in neonatal and surgical care, survival is now greater than 80%.
Possible Complications
Lung infections
Other congenital problems
When to Contact a Medical Professional
Go to the emergency room or call the local emergency number (such as 911). A diaphragmatic hernia is a surgical emergency.
An abscess is an infection characterized by a collection of pus underneath a portion of the skin. Bacteria commonly causing abscesses are Staphylococcus aureus and Streptococcus. These bacteria enter the skin through any cracks or injury to the skin. That area of skin then becomes red, tender, warm, and swollen over days to 1–2 weeks and a fever may develop. Abscesses can sometimes form if minor superficial skin infections are not treated appropriately and in a timely fashion. Most abscesses resolve quickly once appropriately treated.
Community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) is a strain of "staph" bacteria resistant to antibiotics in the penicillin family, which have been the cornerstone of antibiotic therapy for staph and skin infections for decades. CA-MRSA previously infected only small segments of the population, such as health care workers and persons using injection drugs. However, CA-MRSA is now a common cause of skin infections in the general population. While CA-MRSA bacteria are resistant to penicillin and penicillin-related antibiotics, most staph infections with CA-MRSA can be easily treated by health care practitioners using local skin care and commonly available non-penicillin-family antibiotics. Rarely, CA-MRSA can cause serious skin and soft tissue (deeper) infections. Staph infections typically start as small red bumps or pus-filled bumps, which can rapidly turn into deep, painful sores. If you see a red bump or pus-filled bump on the skin that is worsening or showing any signs of infection (ie, the area becomes increasingly painful, red, or swollen), see your doctor right away. Many patients believe incorrectly that these bumps are the result of a spider bite when they arrive at the doctor's office. Your doctor may need to test (culture) infected skin for MRSA before starting antibiotics. If you have a skin problem that resembles a CA-MRSA infection or a culture that is positive for MRSA, your doctor may need to provide local skin care and prescribe oral antibiotics. To prevent spread of infection to others, infected wounds, hands, and other exposed body areas should be kept clean and wounds should be covered during therapy.
Factors that predispose individuals to developing an abscess include:
Any skin infection, especially those that are untreated
Diabetes
Obesity
Intravenous drug abuse
Weakened immune system due to underlying illness or medication
Who's At Risk
Abscesses can occur in anyone and occur anywhere on the body.
You might be able to sense fluid in an abscess when you press on the abscess with a finger.
Signs and Symptoms
A worsening red, tender swelling that arises over a period of 1–2 weeks. The pus underneath the skin is usually not visible. You may have a fever or a general sense of not feeling well.
Self-Care Guidelines
There are no self-care options for abscesses. While waiting to see your doctor, you can try applying a warm compress to the affected area and take ibuprofen to help with the swelling and pain.
When to Seek Medical Care
A worsening red, tender swelling should prompt you to make an appointment with your physician as soon as possible. If the area involves your face, is spreading rapidly, or is in an area that severely limits your functionality, you should seek emergency care.
Treatments Your Physician May Prescribe
Your doctor may drain the pus and fluid collection by making a small incision in the skin after it has been numbed. This will drain a majority of the bacteria, helping the body fight the small amount that remains. This fluid may then be sent to a laboratory for testing (culture), but not necessarily. The culture can tell the doctor not only what type of bacterium is causing the infection but also what antibiotics will work best to treat it. This may take as little as 2–3 days. Your doctor may choose to have you start oral antibiotics aimed at treating the most common bacteria that cause abscesses while awaiting these results. However, if the infection is small and it has been drained, your doctor may decide to not treat you with oral antibiotics.
If your symptoms are not improving or it is determined that the bacterium is not one of the common types, your doctor may prescribe different antibiotics. If your doctor prescribes antibiotics, it is important to take the entire course as prescribed, even if you are feeling better or the infection appears to be gone after just a few days. If you have been taking antibiotics and the infection itself or the way you are generally feeling have not improved in about 2–3 days, return to see your doctor.
Желтуха новорожденных – это состояние, при котором у ребенка повышается уровень билирубина в крови. Билирубин – это желтое вещество, образующееся в организме при разрушении старых эритроцитов. Билирубин разрушается в печени и выводится из организма со стулом.
При высоком уровне билирубина в крови происходит окрашивание кожи и склер ребенка в желтый цвет. Это состояние и называется желтухой.
Желтуха новорожденных (желтушная окраска кожи) обусловлена многими причинами, но у большинства детей это состояние называется физиологической желтухой - естественное явление для новорожденного, развивающееся из-за незрелости печени. Этот тип желтухи, как правило, длится всего несколько дней. Ребенок с желтухой должен наблюдаться врачом до снижения или нормализации уровня билирубина в крови.
Незначительное повышение уровня билирубина у младенца сразу после рождения является нормальным явлением.
Когда ребенок растет в утробе матери, плацента удаляет билирубин из организма ребенка. Плацента является органом, который также растет во время беременности и защищает ребенка. После рождения ребенка эту функцию начинает выполнять печень. Для этого может потребоваться некоторое время.
Желтушное окрашивание кожи, или желтуха, появляется у большинства новорожденных. Она называется "физиологической желтухой". Это состояние не опасно, и обычно проявляется на 2-4 день жизни ребенка. Симптомы проходят в течение 2 недель и обычно не вызывают осложнений.
У новорожденных, которых кормят грудью, может возникнуть два типа желтухи. Оба типа, как правило, безопасны.
· Желтуха грудного вскармливания проявляется в течение первой недели жизни, особенно у детей, которые плохо сосут грудь или в тех случаях, когда молоко матери выделяется медленно.
· Желтуха грудного молока может появиться у некоторых здоровых детей, находящихся на грудном вскармливании, после 7-го дня жизни. Она, как правило, достигает максимума на 2-3 неделе жизни ребенка и может продлиться в течение месяца или более. Это состояние может быть связано с влиянием на распад билирубина в печени веществ, содержащихся в грудном молоке. Желтуха грудного молока отличается от желтухи грудного вскармливания.
Тяжелые формы желтухи новорожденных могут возникнуть в случаях, если у вашего ребенка повышается количество эритроцитов, которые должны быть заменены организмом. Это бывает при следующих состояниях:
· Появление аномальных клеток крови
· Несоответствие групп крови у матери и ребенка
· Кровоизлияние между надкостницей и наружной поверхностью черепа (кефалогематома), вызванное трудными родами
· Высокий уровень эритроцитов, что часто встречается у детей с низким гестационным возрастом (соответствует сроку беременности) и у некоторых близнецов
· Инфекции
· Отсутствие или недостаток определенных важных белков (ферментов)
При определенных условиях организму ребенка становится сложно выводить билирубин, что приводит к развитию более тяжелой желтухи. К этим условиям относятся:
· Прием некоторых лекарств
· Врожденные инфекции, такие как краснуха, сифилис и другие
· Болезни, поражающие печень или желчные пути, такие как муковисцидоз или гепатит
· Низкий уровень кислорода (гипоксия)
· Инфекции (например, сепсис)
· Множество различных генетических или наследственных заболеваний
У детей, родившихся преждевременно, желтуха развивается чаще, чем у доношенных.
При желтухе кожа окрашивается в желтый цвет. Желтушное окрашивание начинается с лица, а затем спускается вниз к груди, к области живота, ногам и стопам.
Иногда у детей с выраженной желтухой имеются повышенная утомляемость и плохой аппетит.
Врачи, медсестры и члены семьи наблюдают за признаками желтухи в роддоме и после выписки новорожденного домой.
Каждому ребенку с желтухой необходимо сразу измерить уровень билирубина. Для этого необходимо взять кровь на анализ.
Во многих больницах уровень общего билирубина определяется у всех детей в первые 24 часа жизни. Для этого используются специальные зонды, которыми можно определить уровень билирубина путем простого прикосновения к коже. Высокие значения необходимо подтвердить с помощью анализов крови.
К необходимым обследованиям относятся:
· Общий анализ крови
· Проба Кумбса
· Определение количества ретикулоцитов
Дальнейшие обследования могут потребоваться для детей, нуждающихся в лечении, или при резком повышении уровня общего билирубина.
· родился ли ребенок преждевременно (детей, рожденных раньше срока, необходимо лечить до снижения уровня билирубина)
· возраст ребенка на данный момент
Ребенок нуждается в лечении, если уровень билирубина слишком высок или быстро нарастает.
Часто кормите ребенка грудным молоком или молочными смесями. Частые кормления (до 12 раз в сутки) стимулируют работу кишечника, тем самым, помогая выведению билирубина со стулом. Проконсультируйтесь с врачом, прежде чем дополнительно ввести прикорм молочной смесью.
Некоторые новорожденные нуждаются в лечении еще до выписки из роддома. Другим может потребоваться возвращение в больницу на несколько дней. Обычно лечение длится от 1 до 2 дней.
Иногда у детей с высоким уровнем билирубина применяется лечение ультрафиолетом. Эта процедура называется фототерапией. Ультрафиолетовые лучи помогают разрушить билирубин в коже.
Младенец находится под лампами искусственного света в теплой, закрытой кровати для поддержания постоянной температуры. На ребенка надевается только подгузник и специальные очки для защиты глаз. Педиатры рекомендуют продолжать грудное вскармливание при фототерапии, если это возможно. В редких случаях ребенку может потребоваться внутривенное введение жидкостей.
Если уровень билирубина не слишком высок или он не нарастает, вы можете проводить фототерапию дома при помощи специального волоконно-оптического одеяла, в котором имеются крошечные, яркие лучи. Вы также можете использовать кровать, рассеивающую свет через матрац.
· При проведении фототерапии вам необходимо кормить ребенка каждые 2-3 часа (от 10 до 12 раз в день).
· Медработник будет приходить к вам домой, чтобы учить вас правильно пользоваться одеялом или кроватью и для того, чтобы контролировать состояние вашего ребенка.
· Медработник будет приходить ежедневно, чтобы измерить вес вашего ребенка, проверить правильность кормления, состояние кожи и уровень билирубина.
· Вам будет предложено подсчитать количество мокрых и грязных подгузников.
В самых тяжелых случаях желтухи может потребоваться обменное переливание крови. Суть процедуры заключается в замене крови ребенка на свежую плазму. У детей с тяжелым течением желтухи для снижения уровня билирубина может быть эффективным внутривенное введение иммуноглобулина.
Обычно желтуха новорожденных не опасна. У большинства детей желтуха обычно проходит без лечения в течение 1-2 недель.
Очень высокий уровень билирубина может повредить мозг. Это состояние называется ядерной желтухой. Однако это состояние почти всегда диагностируется до того, как уровень билирубина становятся настолько высокими, чтобы вызвать повреждение.
Все дети до 5 дня жизни должны быть осмотрены врачом для проверки на наличие желтухи.
Те дети, которые провели меньше 24 часов в роддоме, должны быть осмотрены врачом до возраста 72 часов.
Дети, отправленные домой в промежутке между 24 и 48 часами, осматриваются до возраста 96 часов.
Дети, отправленные домой в промежутке между 48 и 72 часами, осматриваются до возраста 120 часов.
Желтуха опасна, если у ребенка имеется лихорадка (повышенная температура), ребенок стал вялым или плохо ест. Течение желтухи может быть опасным у новорожденных из групп высокого риска.
Как правило, желтуха НЕ опасна для здоровых новорожденных. Обратитесь к педиатру, если:
Течение желтухи тяжелое (кожа ярко-желтой окраски)
Желтуха продолжает нарастать в течение 2-х недель и больше, или развиваются другие симптомы.
Желтуха новорожденных является нормальным явлением и ее невозможно предупредить. Риск развития тяжелой желтухи часто может быть снижен путем частого кормления младенцев, по крайней мере, по 8-12 раз в день в течение первых нескольких дней и путем тщательного выявления детей, подвергающихся наибольшему риску.
Всем беременным женщинам должна быть определена группа крови и выявлены аномальные антитела. Если мать резус - отрицательна, рекомендуется обследование младенца. Обследование также может понадобиться, если группа крови матери О (I)Rh+, но в этом нет необходимости, если ведется тщательный мониторинг.
Тщательный контроль всех младенцев первых 5-ти дней жизни может предотвратить развитие большинства осложнений желтухи. В идеале необходимо:
Помнить о риске развития желтухи у ребенка
Измерять уровень билирубина в первый день жизни ребенка
Запланировать, по крайней мере, одно посещение на дому для детей первой недели жизни, отправленных домой из роддома в течение 72 часов.
Диафрагмальнаягрыжа является врожденным дефектом, при котором в диафрагме - мышце, участвующей в акте дыхания - имеется аномальное отверстие. Открытое отверстие позволяет части органов брюшной полости (желудок, селезенка, печень и кишечник) проникать в грудную полость к легким.
Аномальное отверстие в диафрагме, позволяющее части органов брюшной полости мигрировать в грудную полость, возникает еще до рождения.
Диафрагмальная грыжа обусловлена неправильным соединением анатомических тканей и структур в период внутриутробного развития. В результате органы брюшной полости, такие как желудок, тонкий кишечник, селезенка, часть печени, почки поднимаются в грудную полость. Ткань легких на стороне поражения развивается не полностью.
Врожденная диафрагмальная грыжа проявляется у 1 из 2200-5000 новорожденных. Наиболее часто поражается левая сторона. При наличии у родителей или братьев данной патологии риск возникновения заболевания увеличивается.
Из-за неэффективного движения диафрагмы и сдавления легочной ткани вскоре после рождения ребенка почти всегда развивается коллапс легкого (спадение части легкого), который приводит к тяжелой дыхательной недостаточности.
Другие симптомы:
· Синюшная окраска кожи из-за недостатка кислорода
У беременной женщины может быть избыточное количество амниотической жидкости. Ультразвуковое исследование плода может показать проникновение содержимого брюшной полости в грудную полость.
Обследование младенцев может установить:
· Неправильное движение грудной клетки
· Дыхание не проводится на пораженной стороне
· Перистальтика кишечника слышна в грудной клетке
· При пальпации брюшной полости определяется уменьшение ее объема
На рентгенограмме грудной клетки может быть обнаружено расположение органов брюшной полости в грудной.
Младенцу может понадобиться искусственная поддержка дыхания, пока он не оправится после операции. Некоторые дети находятся на аппарате жизнеобеспечения «искусственное сердце – легкие», что позволяет легким восстановиться и расправиться после операции.
Если диафрагмальная грыжа диагностируется во время беременности (около 24 до 28 недель), могут быть рассмотрены варианты фетального оперативного вмешательства.
Исход операции зависит от того, насколько хорошо развились легкие, а также от того, есть ли какие-либо другие врожденные дефекты. Обычно прогноз благоприятный для детей с достаточным объемом легочной ткани при отсутствии других заболеваний.
Благодаря достижениям в области неонатальной и хирургической помощи выживаемость в настоящее время превышает 80%.
Обратитесь или позвоните в службу оказания экстренной медицинской помощи (например, 103). Диафрагмальная грыжа является показанием для срочного хирургического вмешательства.