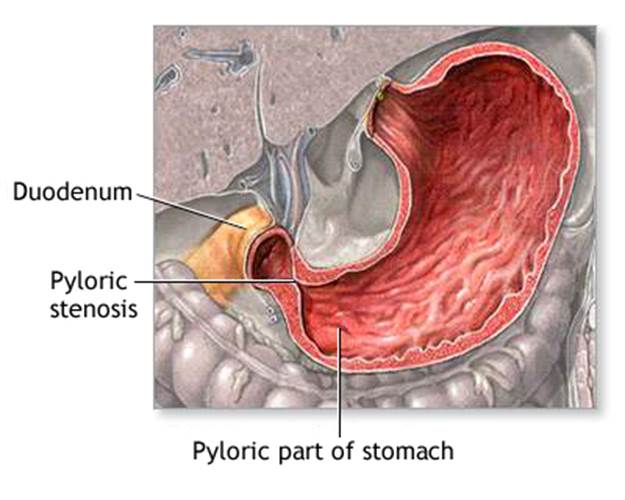
Normally, food passes easily from the stomach into the first part of the small intestine through a valve called the pylorus. With pyloric stenosis, the muscles of the pylorus are thickened. This prevents the stomach from emptying into the small intestine.
The cause of the thickening is unknown. Genes may play a role, since children of parents who had pyloric stenosis are more likely to have this condition.
Pyloric stenosis occurs most often in infants younger than 6 months. It is more common in boys than in girls.
Treatment for pyloric stenosis involves surgery to widen the pylorus. The surgery is called pyloromyotomy.
If putting the infant to sleep for surgery is not safe, a device called an endoscope with a tiny balloon at the end is used. The balloon is inflated to widen the pylorus.
In infants who cannot have surgery, tube feeding or medicine to relax the pylorus is tried.
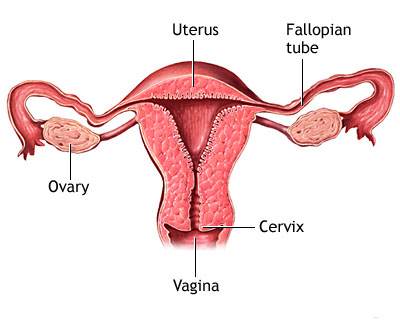
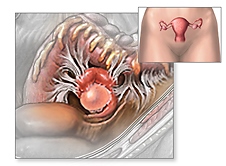
An ovarian cyst is a fluid-filled sac in or on the ovary. There are several types of ovarian cysts. Many ovarian cysts are noncancerous cysts that occur as a result of ovulation (the release of an egg from the ovary). These are called functional cysts.
Often functional cysts do not cause any symptoms (you may not even know you have one), but other times they can cause abdominal pain, bloating, menstrual irregularities, nausea and vomiting. Other symptoms include feeling full after eating just a little and constipation.
If you are menopausal and are not having periods, you shouldn't form functional cysts, but it is possible for you to form other types of ovarian cysts. You should call your doctor if you experience any of the symptoms of an ovarian cyst.
Often times, your doctor will feel a cyst during your physical exam. If you do have a cyst, your doctor will probably want you to have a sonogram so he or she can look at the cyst. What your doctor decides to do after that depends on your age, the way the cyst looks on the sonogram and if you're having symptoms.
A sonogram uses sound waves to make pictures of organs in the body. It's a good way for your doctor to look at your ovaries. This kind of sonogram can be done either through your abdomen or your vagina. Neither type is painful. The sonogram usually lasts about 30 minutes. It will give your doctor valuable information about the size and the appearance of your cyst.
Your doctor might test the level of a protein called CA-125 in your blood. Sometimes this blood test is done in women who have an ovarian cyst to see if their cyst could be cancerous. A normal CA-125 level is less than 35. However, this test is not always an accurate way to tell if a woman has ovarian cancer. For example, some women who do have ovarian cancer have a normal CA-125 level. Also, this level can sometimes be high in women who do not have cancer, particularly if they are in their childbearing years. For these reasons, the CA-125 blood test is only recommended for women who show signs or symptoms of ovarian cancer or who have genetic mutations that increase the risk of ovarian cancer.
Functional cysts normally shrink on their own over time, usually in about 1 to 3 months. If you have a functional cyst, your doctor may want to check you again in 1 to 3 months to make sure the cyst has gotten smaller. If you develop functional cysts often, your doctor may want you to take birth control pills so you won't ovulate. If you don't ovulate, you won't form functional cysts.
The treatment for ovarian cysts depends on several things, such as your age, whether you are having periods, the size of the cyst, its appearance and your symptoms.
If you're having periods, only mild symptoms and the cyst is functional, you probably won't need to have surgery. If the cyst doesn't go away after several menstrual periods, if it gets larger or if it doesn't look like a functional cyst on the sonogram, your doctor may want you to have an operation to remove it. There are many different types of ovarian cysts in women of childbearing age that do require surgery. Fortunately, cysts in women of this age are almost always benign (noncancerous).
If you're past menopause and have an ovarian cyst, your doctor will probably want you to have surgery. Ovarian cancer is rare, but women 50 to 70 years of age are at greater risk. Women who are diagnosed at an early stage do much better than women who are diagnosed later.
If the cyst is small (about the size of a plum or smaller) and if it looks benign on the sonogram, your doctor may decide to do a laparoscopy. This type of surgery is done with a lighted instrument called a laparoscope that's like a slender telescope. This is put into your abdomen through a small incision (cut) just above or just below your navel (belly button). With the laparoscope, your doctor can see your organs. Often the cyst can be removed through small incisions at the pubic hair line.
If the cyst looks too big to remove with the laparoscope or if it looks suspicious in any way, your doctor will probably do a laparotomy. A laparotomy uses a bigger incision to remove the cyst or possibly the entire affected ovary and fallopian tube. While you are under general anesthesia (which puts you in a sleep-like state) the cyst can be tested to find out if it is cancer. If it is cancer, your doctor may need to remove both of the ovaries, the uterus, a fold of fatty tissue called the omentum and some lymph nodes. It's very important that you talk to your doctor about all of this before the surgery. Your doctor will also talk to you about the risks of each kind of surgery, how long you are likely to be in the hospital and how long it will be before you can go back to your normal activities.
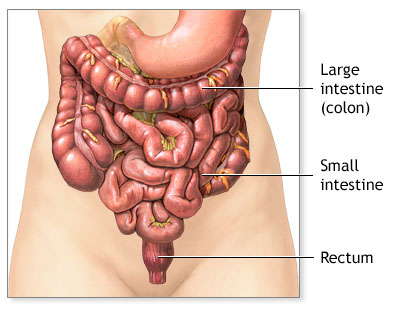
Ulcerative colitis is a type of inflammatory bowel disease (IBD) that affects the lining of the large intestine (colon) and rectum. Crohn's disease is a related condition.
Causes
The cause of ulcerative colitis is unknown. People with this condition have problems with the immune system, but it is not clear whether immune problems cause this illness. Although stress and certain foods can trigger symptoms, they do not cause ulcerative colitis.
Ulcerative colitis may affect any age group, although there are peaks at ages 15 - 30 and then again at ages 50 - 70.
The disease can begin the rectal area, and may involve the entire large intestine over time. It may also start in the rectum and other parts of the large intestine at the same time.
Risk factors include a family history of ulcerative colitis, or Jewish ancestry.
Symptoms
The symptoms vary in severity and may start slowly or suddenly. About half of people only have mild symptoms. Others have more severe attacks that occur more often. Many factors can lead to attacks, including respiratory infections or physical stress.
Colonoscopy with biopsy is generally used to diagnose ulcerative colitis.
Colonoscopy is also used to screen people with ulcerative colitis for colon cancer. Ulcerative colitis increases the risk of colon cancer. If you have this condition, you should be screened with colonoscopy about 8 - 12 years after being diagnosed. You should have a follow-up colonoscopy every 1 - 2 years.
Other tests that may be done to help diagnose this condition include:
Barium enema
Complete blood count (CBC)
C-reactive protein (CRP)
Sedimentation rate (ESR)
Treatment
The goals of treatment are to:
Control the acute attacks
Prevent repeated attacks
Help the colon heal
Hospitalization is often needed for severe attacks. Your doctor may prescribe corticosteroids to reduce inflammation. You may be given nutrients through a vein (intravenous line).
DIET AND NUTRITION
Certain types of foods may worsen diarrhea and gas symptoms, especially during times of active disease. Diet suggestions include:
Eat small amounts of food throughout the day.
Drink plenty of water (drink small amounts throughout the day).
Avoid high-fiber foods (bran, beans, nuts, seeds, and popcorn).
Avoid fatty, greasy or fried foods and sauces (butter, margarine, and heavy cream).
Limit milk products if you are lactose intolerant. Dairy products are a good source of protein and calcium.
STRESS
You may feel worried, embarrassed, or even sad or depresed about having a bowel accident. Other stressful events in your life, such as moving, or losing a job or a loved one can cause digestive problems.
Ask your doctor or nurse for tips on your to manage your stress.
MEDICATION
Medicines that may be used to decrease the number of attacks include:
5-aminosalicylates such as mesalamine or sulfazine, which can help control moderate symptoms
Immunomodulators such as azathioprine and 6-mercaptopurine
Corticosteroids (prednisone and methylprednisolone) taken by mouth during a flare-up or as a rectal suppository, foam, or enema
Infliximab (Remicade) or other biological treatments, if you do not respond to other medications
SURGERY
Surgery to remove the colon will cure ulcerative colitis and removes the threat of colon cancer. Surgery is usually recommended if you have:
Colitis that does not respond to complete medical therapy
Changes in the lining of the colon that are thought to be precancerous
Serious complications such as rupture (perforation) of the colon, severe bleeding (hemorrhage), or toxic megacolon
Most of the time, the entire colon, including the rectum, is removed (total proctocolectomy with ileostomy). Afterwards, you may need a surgical opening in the abdominal wall (ileostomy), or a procedure that connects the small intestine to the anus to gain more normal bowel function.
Outlook (Prognosis)
Symptoms are mild in about half of people with ulcerative colitis. You are less likely to respond well to medicines if your disease is more severe.
Permanent and complete control of symptoms with medications is unusual. Cure is only possible through complete removal of the large intestine.
The risk of colon cancer increases in each decade after ulcerative colitis is diagnosed.
Possible Complications
Repeated swelling (inflammation) leads to thickening of the intestinal wall and rectum with scar tissue. Death of colon tissue or severe infection (sepsis) may occur with severe disease.
The pancreas is an organ located behind the stomach that produces chemicals called enzymes, as well as the hormones insulin and glucagon. Most of the time, the enzymes are only active after they reach the small intestine, where they are needed to digest food.
When these enzymes somehow become active inside the pancreas, they eat (and digest) the tissue of the pancreas. This causes swelling, bleeding (hemorrhage), and damage to the pancreas and its blood vessels.
Acute pancreatitis affects men more often than women. Certain diseases, surgeries, and habits make you more likely to develop this condition.
The condition is most often caused by alcoholism and alcohol abuse (70% of cases in the United States). Genetics may be a factor in some cases. Sometimes the cause is not known, however.
Other conditions that have been linked to pancreatitis are:
Autoimmune problems (when the immune system attacks the body)
Blockage of the pancreatic duct or common bile duct, the tubes that drain enzymes from the pancreas
Damage to the ducts or pancreas during surgery
High blood levels of a fat called triglycerides (hypertriglyceridemia)
Injury to the pancreas from an accident
Other causes include:
Complications of cystic fibrosis
Hemolytic uremic syndrome
Hyperparathyroidism
Kawasaki disease
Reye syndrome
Use of certain medications (especially estrogens, corticosteroids, thiazide diuretics, and azathioprine)
Viral infections, including mumps, coxsackie B, mycoplasma pneumonia, and campylobacter
Laboratory tests will be done. Tests that show the release of pancreatic enzymes include:
Increased blood amylase level
Increased serum blood lipase level
Increase urine amylase level
Other blood tests that can help diagnose pancreatitis or its complications include:
Complete blood count (CBC)
Comprehensive metabolic panel
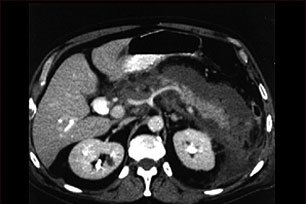
Imaging tests that can show inflammation of the pancreas include:
Abdominal CT scan
Abdominal MRI
Abdominal ultrasound
Treatment
Treatment often requires a stay in the hospital and may involve:
Pain medicines
Fluids given through a vein (IV)
Stopping food or fluid by mouth to limit the activity of the pancreas
Occasionally a tube will be inserted through the nose or mouth to remove the contents of the stomach (nasogastric suctioning). This may be done if vomiting or severe pain do not improve, or if a paralyzed bowel (paralytic ileus) develops. The tube will stay in for 1 - 2 days to 1 - 2 weeks.
Treating the condition that caused the problem can prevent repeated attacks.
In some cases, therapy is needed to:
Drain fluid that has collected in or around the pancreas
A peptic ulcer is a defect in the lining of the stomach or the first part of the small intestine, an area called the duodenum.
A peptic ulcer in the stomach is called a gastric ulcer. An ulcer in the duodenum is called a duodenal ulcer.
Causes
Normally, the lining of the stomach and small intestines is protected against the irritating acids produced in your stomach. If this protective lining stops working correctly and the lining breaks down, it results in inflammation (gastritis) or an ulcer.
Most ulcers occur in the first layer of the inner lining. A hole that goes all the way through the stomach or duodenum is called a perforation. A perforation is a medical emergency.
The most common cause of such damage is infection of the stomach by bacteria called Helicobacter pylori(H.pylori). Most people with peptic ulcers have these bacteria living in their gastrointestinal (GI) tract. Yet, many people who have these bacteria in their stomach do not develop an ulcer.
The following also raise your risk for peptic ulcers:
Drinking too much alcohol
Regular use of aspirin, ibuprofen, naproxen, or other nonsteroidal anti-inflammatory drugs (NSAIDs). Taking aspirin or NSAIDs once in a while is safe for most people.
Smoking cigarettes or chewing tobacco
Being very ill, such as being on a breathing machine
Having radiation treatments
A rare condition called Zollinger-Ellison syndrome causes stomach and duodenal ulcers. Persons with this disease have a tumor in the pancreas. This tumor releases high levels of a hormone that increases stomach acid.
Many people believe that stress causes ulcers. It is not clear if this is true, at least for everyday stress at home.
SYMPTOMS
Small ulcers may not cause any symptoms. Some ulcers can cause serious bleeding.
Abdominal pain is a common symptom, but it doesn't always occur. The pain can differ from person to person.
Other symptoms include:
Feeling of fullness -- unable to drink as much fluid
Hunger and an empty feeling in the stomach, often 1 - 3 hours after a meal
To diagnose an ulcer, your doctor will order one of the following tests:
Esophagogastroduodenoscopy (EGD or upper endoscopy) is a special test performed by a gastroenterologist. A thin tube with a camera on the end is inserted through your mouth into the GI tract to see your stomach and small intestine.
Upper GI is a series of x-rays taken after you drink a thick substance called barium.
Upper endoscopy is also done on people who are at high risk for stomach cancer. Risk factors include being over age 45 or having symptoms such as:
Treatment involves a combination of medications to kill the H. pylori bacteria (if present), and reduce acid levels in the stomach. This strategy allows your ulcer to heal and reduces the chance it will come back.
Take all of your medications exactly as prescribed.
If you have a peptic ulcer with an H. pylori infection, the standard treatment uses different combinations of the following medications for 5 - 14 days:
Two different antibiotics to kill H. pylori, such as clarithromycin, amoxicillin, tetracycline, or metronidazole
Proton pump inhibitors such as omeprazole, lansoprazole, or esomeprazole
Bismuth may be added to help kill the bacteria
If you have an ulcer without an H. pylori infection, or one that is caused by taking aspirin or NSAIDs, your doctor will likely prescribe a proton pump inhibitor for 8 weeks.
You may also be prescribed this type of medicine if you must continue taking aspirin or NSAIDs for other health conditions.
PROGNOSIS
Peptic ulcers tend to come back if untreated. If you follow your doctor's treatment instructions and take all of your medications as directed, the H. pylori infection will likely be cured and you'll be much less likely to get another ulcer.
POSSIBLE COMPLICATIONS
Bleeding inside the body (internal bleeding)
Gastric outlet obstruction
Inflammation of the tissue that lines the wall of the abdomen (peritonitis)
Perforation of the stomach and intestines
WHEN TO CONTACT A DOCTOR
Seek urgent help if you:
Develop sudden, sharp abdominal pain
Have a rigid, hard abdomen that is tender to touch
Have symptoms of shock such as fainting, excessive sweating, or confusion
Vomit blood or have blood in your stool (especially if it's maroon or dark, tarry black)
Call your doctor if:
You feel dizzy or light-headed
You have ulcer symptoms
PREVENTION
Avoid aspirin, ibuprofen, and other NSAIDs. Try acetaminophen instead. If you must take such medicines, talk to your doctor first. Your doctor may:
Test you for H. pylori first
Have you take proton pump inhibitors (PPIs) or an acid blocker
Have you take a drug called misoprostol
The following lifestyle changes may help prevent peptic ulcers: