Транзиторлық ишемиялық шабуыл (ТИШ) – мидағы қан айналымының қысқа мерзімді бұзылысы. Кейде микроинсульт аталады. Алайда, инсульттен айырмашылығы (мидың қанмен қамтамасыз етілуінің тоқтауы) транзиторлық ишемиялық шабуылдың симптомдары басылғаннан бір сағаттан кейін жойылады.
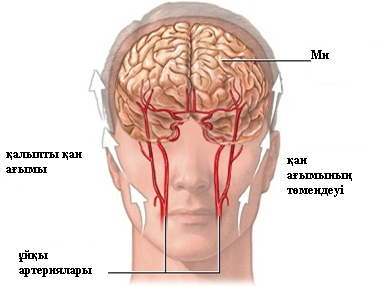
Мида қан келудің негізгі ағыны мойын аумағында орналасқан артериялар (ұйқы артериясы) арқылы жүзеге асырылады. ТИШ мидың белгілі бір бөлігіне қанның келуінің уақтыша азаюынан туындайды. Көбінесе, қан ағымы қантамырларының ұсақ қан ұйындыларынан тежелу салдарынан төмендейді, қан ұйындылары миға қан келуін және қоректік заттектердің түсуін уақытша тежейді. Мидың қанмен қамтамасыз етілуінің уақытша бұзылысы кезінде оның қызметінің күрт бұзылысы орын алады.
ТИШ кезінде мидың қайтымсыз зақымдануы болмайды. Бірақ, алаңдау қажет, себебі, бірінші ұстамасынан кейін екінші, үшінші болуы, инсульт те болуы мүмкін.
ТИШ симптомдарының себебі — мидың жергілікті ишемиясы (қан жетіспеуі), нәтижесінде ишемия даму орнына байланысты ошақтық симптомдар пайда болады.
Ишемияның даму үшін көптеген алғы шарттар болады, олар мидың қантамырларының жағдайына әсер етеді.
ТИШ, әдетте, бірнеше минуттан 1 сағатқа дейін созылуы мүмкін, және көпшілік симптомдар бір сағаттан кейін жойылады. Науқаста шабуылдар бірінен соң бірі пайда болуы мүмкін — мұндай жағдайдағы симптомдар:
· Қозғалудың бұзылысы, бас айналуы
· Ұйқы басуы, сигналдарға нашар серпін, естің бұзылысы немесе тіпті, коматозды жағдай
· Дененің бір немесе бірнеше бөлігінде ұйып, жансыздануы
· Көңіл-күй бұзылысы, нашарлауы
· Сөзді түсінуде және айтудағы қиындықтар
· Дененің бір бөлігіндегі әлсіздік.
ТИШ болған науқаста беттің ассимметриялығы (біркелкі еместігі), ауыз бен көз бұлшық етінің енжарлығы байқалады. Кейбір жағдайда зақымданған адам қолын жоғары көтеріп ұстай алмайды. Сөйлеу айқын болмайды.
Егер миға ұзақ уақыт бойы қан түспесе, немесе симптомдардың ұзақтығы 24 сағаттан асатын болса, шабуыл инсульт саналады. Егер біреуде ТИШ байқасаңыз, жоғарыда келтірілген белгілердің болуын тексеріңіз.
Диагноз қою күрделілігі бұл жағдайда дәрігер анықтап үлгеруі үшін ТИШ аз уақытқа созылуында. Дәрігер инсульт және ТИШ пайда болуымен байланысты қауіп факторларының болуын міндетті түрде тексереді. Кейде неврологиялық тексеру жүргізіледі.
Қарау кезінде дәрігер жүректің жағдайын тексеріп, артериалдық қысымды өлшейді. Сондай-ақ, жүйке жүйесінің, бұлшық еттің жағдайы бағаланады. Сондай-ақ, дәрігер стетоскоптың көмегімен ұйқы артериясын тыңдап, қан ағымының бұзылысымен байланысты шуылды анықтайды.
Нақты диагнозды қойып, инсульт болуын анықтау үшін дәрігер келесі зерттеулерді жүргізеді:
· КТС (компьютерлік-томографиялық сканерлеу, ангиография) — мидың және мойынның артерияларының жағдайын анықтау үшін жүргізіледі. Қантамырға контрастылық заттек енгізіледі, сканерлеуді жеңілдету үшін;
· ЭКГ (электрокардиограмма) — жүректің кез келген қалыпсыз ырғағын анықтауға көмектесетін тест. ЭКГ кезінде науқасқа жүректің электр белсенділігін анықтау үшін электродтар бекітіледі;
· МРТ (магниттік-резонанстық томография) — радиотолқындар және магнит өрісінің көмегімен ішкі ағзалардың бейнесін алу үрдісі.
Инсульт кезінде. Әдетте, мидың бұзылыстары анықталады, ал ТИШ кезінде мұндай өзгерістер анықталмайды.
Жарамды емдеуді таңдау көптеген факторларға байланысты: науқастың жасы, аурудың тарихы, кейбір белгілері мен симптомдарының сипаттамасы.
Дұрыс және тиімді емдеу ТИШ қайталану немесе инсульт болу қаупін едәуір азайтады.
Дәрігер дәрі тағайындайды. Олардың ішінде: анти-тромбоцитарлық (қан ұйындысы түзілуінің алдын алатын) препараттар, мысалы, аспирин немесе клопидогрель негізіндегі (Плавикс) препараттар – қан ұюын бақылау үшін, гипертонияны емдейтін препараттар, сондай-ақ, холестеринді азайтатын дәрілер.
ТИШ – шұғыл медициналық жәрдемді қажет етеді. Симптомдар пайда болысымен Жедел жәрдемді шақырыңыз. Симптомдар өздігінше өткендігіне қарамастан, оларға міндетті түрде назар аудару қажет.
Алайда, ТИШ - нағыз инсульттің жуырдағы күндерде немесе айларда болуының мүмкіндігінің маңызды ескерту дабылы. ТИШ болған адамдардың 10 пайызынан астамында 3 айдың ішінде инсульт дамиды. Бұл жағдайлардың жартысында жақын арадағы 48 сағат ішінде болады. Инсульт сол күні немесе кешірек болуы мүмкін. Кейбір адамдарда бір, басқаларда бірнеше көрінісі болуы мүмкін.
Encephalitis is a rare condition. It occurs more often in the first year of life and decreases with age. The very young and older adults are more likely to have a severe case.
Encephalitis is most often caused by a viral infection. Many types of viruses may cause it. Exposure to viruses can occur through:
· Breathing in respiratory droplets from an infected person
· Contaminated food or drink
· Mosquito, tick, and other insect bites
· Skin contact
Different viruses occur in different locations. Many cases occur during a certain season.
Encephalitis caused by the herpes simplex virus is the leading cause of more severe cases in all ages, including newborns.
Routine vaccination has greatly reduced encephalitis due to some viruses, including:
The outcome varies. Some cases are mild and short, and the person fully recovers. Other cases are severe, and permanent problems or death is possible.
The acute phase normally lasts for 1 to 2 weeks. Fever and symptoms gradually or suddenly disappear. Some people may take several months to fully recover.
Children and adults should avoid contact with anyone who has encephalitis.
Controlling mosquitoes (a mosquito bite can transmit some viruses) may reduce the chance of some infections that can lead to encephalitis.
· Apply an insect repellant containing the chemical, DEET when you go outside (but do not use DEET products on infants younger than 2 months).
· Remove any sources of standing water (such as old tires, cans, gutters, and wading pools).
· Wear long-sleeved shirts and pants when outside, especially at dusk.
Children and adults should get routine vaccinations for viruses that can cause encephalitis. People should receive specific vaccines if they are traveling to places such as parts of Asia, where Japanese encephalitis is found.
Vaccinate animals to prevent encephalitis caused by the rabies virus.
Death is possible in people with a severe pulmonary embolism.
Blood thinners may be prescribed to help prevent DVT in people at high risk, or those who are undergoing high-risk surgery.
If you had a DVT, your provider will prescribe pressure stockings. Wear them as instructed. They will improve blood flow in your legs and reduce your risk of blood clots.
Moving your legs often during long plane trips, car trips, and other situations in which you are sitting or lying down for long periods can also help prevent DVT. People at very high risk for blood clots may need shots of a blood thinner called heparin when they take a flight that lasts longer than 4 hours.
Do not smoke. If you smoke, quit. Women who are taking estrogen must stop smoking. Smoking increases your risk of developing blood clots.
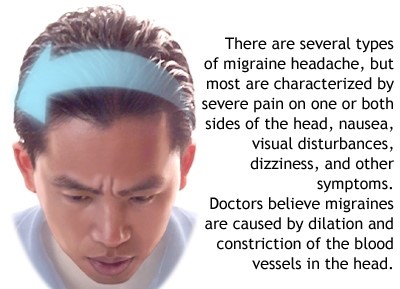
A migraine is a common type of headache that may occur with symptoms such as nausea, vomiting, or sensitivity to light. In many people, a throbbing pain is felt only on one side of the head.
Some people who get migraines have warning symptoms, called an aura, before the actual headache begins. An aura is a group of symptoms, including vision disturbances, that are a warning sign that a bad headache is coming.
Symptoms of a migraine attack may include heightened sensitivity to light and sound, nausea, auras (loss of vision in one eye or tunnel vision), difficulty of speech and intense pain predominating on one side of the head.
Migraine headaches tend to first appear between the ages of 10 and 45. Sometimes they may begin later in life.
Migraines occur more often in women than men
Migraines may run in families
Some women, but not all, may have fewer migraines when they are pregnant
A migraine is caused by abnormal brain activity, which can be triggered by a number of factors. However, the exact chain of events remains unclear. Today, most medical experts believe the attack begins in the brain, and involves nerve pathways and chemicals. The changes affect blood flow in the brain and surrounding tissues.
Alcohol, stress and anxiety, certain odors or perfumes, loud noises or bright lights, and smoking may trigger a migraine. Migraine attacks may also be triggered by:
Caffeine withdrawal
Changes in hormone levels during a woman's menstrual cycle or with the use of birth control pills
Changes in sleep patterns
Exercise or other physical stress
Missed meals
Smoking or exposure to smoke
Migraine headaches can be triggered by certain foods. The most common are:
Any processed, fermented, pickled, or marinated foods, as well as foods that contain monosodium glutamate (MSG)
Baked goods, chocolate, nuts, peanut butter, and dairy products
Foods containing tyramine, which includes red wine, aged cheese, smoked fish, chicken livers, figs, and certain beans
Fruits (avocado, banana, citrus fruit)
Meats containing nitrates (bacon, hot dogs, salami, cured meats)
Onions
This list may not include all triggers.
True migraine headaches are not a result of a brain tumor or other serious medical problem. However, only an experienced health care provider can determine whether your symptoms are due to a migraine or another condition.
Vision disturbances, or aura, are considered a "warning sign" that a migraine is coming. The aura occurs in both eyes and may involve any or all of the following:
A temporary blind spot
Blurred vision
Eye pain
Seeing stars or zigzag lines
Tunnel vision
Other warning signs include yawning, difficulty concentrating, nausea, and trouble finding the right words.
Not every person with migraines has an aura. Those who do usually develop one about 10 - 15 minutes before the headache. However, an aura may occur just a few minutes to 24 hours beforehand. A headache may not always follow an aura.
Migraine headaches can be dull or severe. The pain may be felt behind the eye or in the back of the head and neck. For many patients, the headaches start on the same side each time. The headaches usually:
Feel throbbing, pounding, or pulsating
Are worse on one side of the head
Start as a dull ache and get worse within minutes to hours
Last 6 to 48 hours
Other symptoms that may occur with the headache include:
Chills
Increased urination
Fatigue
Loss of appetite
Nausea and vomiting
Numbness, tingling, or weakness
Problems concentrating, trouble finding words
Sensitivity to light or sound
Sweating
Symptoms may linger even after the migraine has gone away. Patients with migraine sometimes call this a migraine "hangover." Symptoms can include:
Feeling mentally dull, like your thinking is not clear or sharp
Your doctor can diagnose this type of headache by asking questions about your symptoms and family history of migraines. A complete physical exam will be done to determine if your headaches are due to muscle tension, sinus problems, or a serious brain disorder.
There is no specific test to prove that your headache is actually a migraine. However, your doctor may order a brain MRI or CT scan if you have never had one before or if you have unusual symptoms with your migraine, including weakness, memory problems, or loss of alertness.
An EEG may be needed to rule out seizures. A lumbar puncture (spinal tap) might be done.
Treatment
There is no specific cure for migraine headaches. The goal is to treat your migraine symptoms right away, and to prevent symptoms by avoiding or changing your triggers.
A key step involves learning how to manage your migraines at home. A headache diary can help you identify your headache triggers. Then you and your doctor can plan how to avoid these triggers.
If you have frequent migraines, your doctor may prescribe medicine to reduce the number of attacks. You need to take the medicine every day for it to be effective. Medications may include:
Antidepressants such as amitriptyline or venlafaxine
Blood pressure medicines such as beta blockers (propanolol) or calcium channel blockers (verapamil)
Seizure medicines such as valproic acid, gabapentin, and topiramate
Botulinum toxin (Botox) injections may also help reduce migraine attacks.
Other medicines are taken at the first sign of a migraine attack. Over-the-counter pain medications such as acetaminophen, ibuprofen, or aspirin are often helpful when your migraine is mild. Be aware, however, that:
Taking medicines more than 3 days a week may lead to rebound headaches -- headaches that keep coming back.
Taking too much acetaminophen can damage your liver. Too much ibuprofen or aspirin can irritate your stomach.
If these treatments don't help, ask your doctor about prescription medicines. These include nasal sprays, suppositories, or injections. Your doctor can select from several different types of medications, including:
Triptans -- prescribed most often for stopping migraine attacks
Ergots -- contain different forms of ergotamine
Isometheptene (Midrin)
Some migraine medicines narrow your blood vessels. If you are at risk for heart attacks or have heart disease, talk with your health care provider before using these medicines. Do not take ergots if you are pregnant or planning to become pregnant.
Other medications are given to treat the symptoms of migraine. They may be used alone or along with other drugs. Medications in this group include:
Nausea medicines
Sedatives such as butalbital
Narcotic pain relievers
Feverfew is a popular herb for migraines. Several studies, but not all, support using feverfew for treating migraines. If you are interested in trying feverfew, make sure your doctor approves. Also, know that herbal remedies sold in drugstores and health food stores are not regulated. Work with a trained herbalist when selecting herbs.
Every person responds differently to treatment. Some people have rare headaches that need little to no treatment. Others need to take several medications or even go to the hospital sometimes.
Migraine headache is a risk factor for stroke in both men and women. The risk is higher in people who have migraines that occur with aura. People with migraines should avoid other risk factors for stroke, include smoking, taking birth control pills, and eating an unhealthy diet.
When to Contact a Medical Professional
Call Emergency if:
You are experiencing "the worst headache of your life"
You have speech, vision, or movement problems or loss of balance, especially if you have not had these symptoms with a migraine before
Your headaches are more severe when lying down
The headache starts very suddenly
Also, call your doctor if:
Your headache patterns or pain change
Treatments that once worked are no longer helpful
You have side effects from medication, including irregular heartbeat, pale or blue skin, extreme sleepiness, persistent cough, depression, fatigue, nausea, vomiting, diarrhea, constipation, stomach pain, cramps, dry mouth, or extreme thirst
You are pregnant or could become pregnant -- some medications should not be taken when pregnant
See the general article on headaches for more information on emergency symptoms
Алып жасушалы артериит (АЖА) – бұл егде жастағы адамдарда орташа және ірі артериялардың жүйелі қабыну ауруы, бас ауыруымен және тұмаудағыдай симптомдармен қосарланады. Сондай-ақ, ол самайлық немесе краниалдық артериит (Хортон ауруы) ретінде де белгілі.
Алып жасушалы артериит беткері самайлық артерияның ісінуін және қалыңдауын туындатуы мүмкін. Беткері самайлық артерия – бұл сыртқы ұйқы артериясының жұқа соңғы сағасы.
Ауру тек 50 жастан асқан ересектерде пайда болады, негізінен, егде жастағы адамдарды зақымдайды, көбінесе, ерлерге қарағанда әйелдер жиі шалдығады.
АЖА кезінде бассүйектің артериялары, көбінесе, самай артериялары, сондай-ақ, көздің артериялары зақымданады, демек АЖА көздің көрмеуіне апаруы мүмкін. Көруді жоғалтуды уақытылы анықтаумен және емдеумен алдын алуға болады.
Аурудың бастапқы кезінде диагнозды қою қиын, себебі, бұл ауру туралы мәліметтер аз.
Бастың артерияларының беткері артериялары ұзындығы бойына біркелкі емес түрде тығыздалады, иректеліп, дөңестенеді, үстінен басқанда жалпақ түрге ауыспайды.
Егде жастағы науқастың жалпы қан талдауында:
эритроциттердің шөгу жылдамдығының күрт артуы (СОЭ > 50 мм/ч)
гипохромдық анемия.
Диагнозды нақтылау үшін өткізу қажет:
контрастылық заттекті енгізумен самай артериясының рентгенологиялық зерттеуі (самай артериясының ангиографиясы)
зақымданған самайлық және/немесе басқа артерияның биопсиясы (анықтау мақсатында организмнен тіршілік етуінде жасушаларды немесе тіндерді (биоптат) алу әдісі), әрі қарай тіннің үлгісіне микроскопиялық зерттеу жүргізіледі
офтальмоскопия – арнайы аспаптар (офтальмоскоп немесе фундус-линзалар) көмегімен көз түбін қарау, бұл торқабықты, көру нервісінің дискін, көз түбінің тамырларын бағалауға мүмкіндік береді).
Емдеуді ерте бастау қажет, себебі, ауру көруді жоғалтуға апаруы мүмкін.
Бүгінде АЖА емдеудің ең тиімді тәсілі - кортикостероидтарды (гормондарды) қолдану. Емдеу схемасын дәрігер тағайындайды. АЖА күмән болса да гормондарды тағайындау негізделген. Әдетте, емдеу басталғаннан кейін симптомдар тез жойылады.
АЖА кезінде науқастар үшін болжамы - оң. Әдетте, ауру өлім-жітімге апармайды. Аурудың барысы меңдейді, бірақ, уақытылы басталған емдеу науқастың жағдайын тұрақтандырады.

 Ниже приведены рекомендации по профилактике и выявлению причин возникновения
Ниже приведены рекомендации по профилактике и выявлению причин возникновения