В журнале Neurology опубликованы результаты исследования, доказывающего, что знание еще одного языка, помимо родного, значительно снижает риск развития заболеваний, ведущих к деградации функций головного мозга.
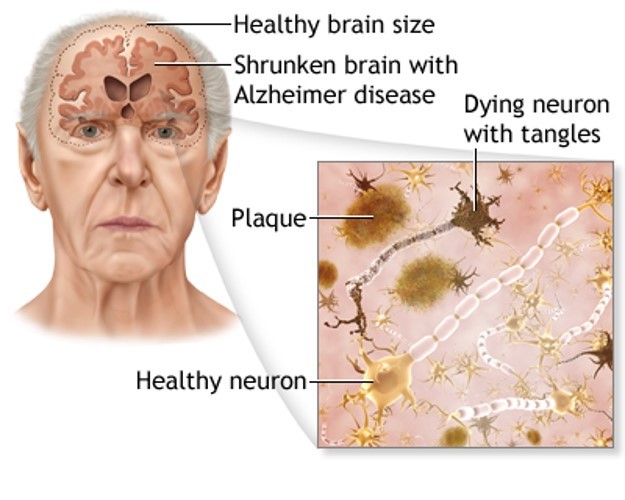
Dementia is a loss of brain function that occurs with certain diseases. Alzheimer disease is one form of dementia. It affects memory, thinking, and behavior.
The exact cause of Alzheimer disease (AD) is not known. Research shows that certain changes in the brain lead to AD.
You are more likely to develop AD if you:
Are older. Developing AD is not a part of normal aging.
Have a close relative, such as a brother, sister, or parent with AD.
Have certain genes linked to AD.
The following may also increase the risk:
Being female
Having heart and blood vessel problems due to high cholesterol
History of head trauma
There are two types of AD:
Early onset AD. Symptoms appear before age 60. This type is much less common than late onset. It tends to get worse quickly. Early onset disease can run in families. Several genes have been identified.
Late onset AD. This is the most common type. It occurs in people age 60 and older. It may run in some families, but the role of genes is less clear.
AD symptoms include difficulty with many areas of mental function, including:
Emotional behavior or personality
Language
Memory
Perception
Thinking and judgment (cognitive skills)
AD usually first appears as forgetfulness.
Mild cognitive impairment (MCI) is the stage between normal forgetfulness due to aging, and the development of AD. People with MCI have mild problems with thinking and memory that do not interfere with daily activities. They are often aware of the forgetfulness. Not everyone with MCI develops AD.
Symptoms of MCI include:
Difficulty performing more than one task at a time
Difficulty solving problems
Forgetting recent events or conversations
Taking longer to perform more difficult activities
Early symptoms of AD can include:
Difficulty performing tasks that take some thought, but used to come easily, such as balancing a checkbook, playing complex games (bridge), and learning new information or routines
Getting lost on familiar routes
Language problems, such as trouble remembering the names of familiar objects
Losing interest in things previously enjoyed and being in a flat mood
Misplacing items
Personality changes and loss of social skills
As AD becomes worse, symptoms are more obvious and interfere with the ability to take care of oneself. Symptoms may include:
Change in sleep patterns, often waking up at night
Delusions, depression, and agitation
Difficulty doing basic tasks, such as preparing meals, choosing proper clothing, and driving
Difficulty reading or writing
Forgetting details about current events
Forgetting events in one's life history and losing self-awareness
Hallucinations, arguments, striking out, and violent behavior
Poor judgment and loss of ability to recognize danger
Using the wrong word, mispronouncing words, or speaking in confusing sentences
Withdrawing from social contact
People with severe AD can no longer:
Recognize family members
Perform basic activities of daily living, such as eating, dressing, and bathing
A skilled health care provider can often diagnose AD with the following steps:
Performing a complete physical exam, including a nervous system exam
Asking about the person's medical history and symptoms
Mental function tests (mental status examination)
A diagnosis of AD is made when certain symptoms are present, and by making sure other causes of dementia are not present.
Tests may be done to rule out other possible causes of dementia, including:
Anemia
Brain tumor
Chronic infection
Intoxication from medicines
Severe depression
Increased fluid on the brain (normal pressure hydrocephalus)
Stroke
Thyroid disease
Vitamin deficiency
CT or MRI of the brain may be done to look for other causes of dementia, such as a brain tumor or stroke. Sometimes, a PET scan can be used to rule out AD.
The only way to know for certain that someone has AD is to examine a sample of their brain tissue after death.
There is no cure for AD. The goals of treatment are:
Slow the progression of the disease (although this is difficult to do)
Manage symptoms, such as behavior problems, confusion, and sleep problems
Change the home environment to make daily activities easier
Support family members and other caregivers
Medicines are used to:
Slow the rate at which symptoms worsen, though the benefit from using these drugs may be small
Control problems with behavior, such as loss of judgment or confusion
Before using these medicines, ask the provider:
What are the side effects? Is the medicine worth the risk?
When is the best time, if any, to use these medicines?
Do medicines for other health problems need to be changed or stopped?
Someone with AD will need support in the home as the disease gets worse. Family members or other caregivers can help by helping the person cope with memory loss and behavior and sleep problems. It is important to make sure the home of a person who has AD is safe for them.
Having AD or caring for a person with the condition may be a challenge. You can ease the stress of illness by seeking support through AD resources. Sharing with others who have common experiences and problems can help you not feel alone.
How quickly AD gets worse is different for each person. If AD develops quickly, it is more likely to worsen quickly.
People with AD often die earlier than normal, although a person may live anywhere from 3 to 20 years after diagnosis.
Families will likely need to plan for their loved one's future care.
The final phase of the disease may last from a few months to several years. During that time, the person becomes totally disabled. Death usually occurs from an infection or organ failure.
Amnesia refers to the loss of memories, such as facts, information and experiences. Though having no sense of who you are is a common plot device in movies and television, real-life amnesia generally doesn't cause a loss of self-identity.
Instead, people with amnesia — also called amnestic syndrome — are usually lucid and know who they are, but may have trouble learning new information and forming new memories.
Amnesia can be caused by damage to areas of the brain that are vital for memory processing. Unlike a temporary episode of memory loss (transient global amnesia), amnesia can be permanent.
There's no specific treatment for amnesia, but techniques for enhancing memory and psychological support can help people with amnesia and their families cope.
The two main features of amnesia are:
Impaired ability to learn new information following the onset of amnesia (anterograde amnesia)
Impaired ability to recall past events and previously familiar information (retrograde amnesia)
Most people with amnesia have problems with short-term memory — they can't retain new information. Recent memories are most likely to be lost, while more remote or deeply ingrained memories may be spared. Someone may recall experiences from childhood or know the names of past presidents, but not be able to name the current president or remember what month it is or what was for breakfast.
Isolated memory loss doesn't affect a person's intelligence, general knowledge, awareness, attention span, judgment, personality or identity. People with amnesia usually can understand written and spoken words and can learn skills such as bike riding or piano playing. They may understand they have a memory disorder.
Amnesia isn't the same as dementia. Dementia often includes memory loss, but it also involves other significant cognitive problems that lead to a decline in the ability to carry out daily activities.
A pattern of forgetfulness is also a common symptom of mild cognitive impairment (MCI), but the memory and other cognitive problems in MCI aren't as severe as those experienced in dementia.
Anyone who experiences unexplained memory loss, head injury, confusion or disorientation requires immediate medical attention.
A person with amnesia may not be able to identify his or her location or have the presence of mind to seek medical care. If someone you know has symptoms of amnesia, help the person get medical attention.
Normal memory function involves many parts of the brain, and any disease or injury that affects the brain can interfere with the intricacies of memory.
Amnesia can result from damage to brain structures that form the limbic system, which controls your emotions and memories. These structures include the thalamus, which lies deep within the center of your brain, and the hippocampal formations, which are situated within the temporal lobes of your brain.
Amnesia caused by brain injury or damage is known as neurological amnesia. Possible causes of neurological amnesia include:
Stroke
Brain inflammation (encephalitis) as a result of infection with a virus such as herpes simplex virus, as an autoimmune reaction to cancer somewhere else in the body (paraneoplastic limbic encephalitis), or as an autoimmune reaction in the absence of cancer
Lack of adequate oxygen in the brain, for example, from heart attack, respiratory distress or carbon monoxide poisoning
Long-term alcohol abuse leading to thiamin (vitamin B-1) deficiency (Wernicke-Korsakoff syndrome)
Tumors in areas of the brain that control memory
Degenerative brain diseases, such as Alzheimer's disease and other forms of dementia
Seizures
Certain medications, such as benzodiazepines
Head injuries that cause a concussion, whether from a car accident or sports, can lead to confusion and problems remembering new information. This is especially common in the early stages of recovery. But head injuries usually don't cause severe amnesia.
Another rare type of amnesia, called dissociative (psychogenic) amnesia, stems from emotional shock or trauma, such as being the victim of a violent crime. In this disorder, a person may lose personal memories and autobiographical information, but usually only briefly.
The chance of developing amnesia might increase if you've experienced:
Brain surgery, head injury or trauma
Stroke
Alcohol abuse
Seizures
Amnesia varies in severity and scope, but even mild amnesia takes a toll on daily activities and quality of life. The syndrome can cause problems at work, at school and in social settings.
It may not be possible to recover lost memories. Some people with severe memory problems need to live in a supervised situation or extended-care facility.
You're likely to start by seeing your family doctor or a general practitioner. However, you may then be referred to a doctor who specializes in disorders of the brain and nervous system (neurologist).
It's a good idea to arrive at your appointment well-prepared. Here's some information to help you get ready for your appointment and to know what to expect from your doctor.
Write down any unusual symptoms as you experience them, including any that may seem unrelated to the reason for which you scheduled the appointment.
Write down key personal information, including any major stresses or recent life changes you can recall. Ask family members or friends to help you, to ensure your list is complete.
Make a list of all medications, vitamins or supplements you're taking.
Ask a family member or friend to come with you. Even in the best circumstances, it can be difficult to remember all of the information provided to you during an appointment. Someone with you can help you remember everything that was said.
Bring a notepad and pen or pencil to jot down the points you want to be sure to remember later.
Write down questions to ask your doctor.
Preparing a list of questions can help you make the most of your time with your doctor, as well as ensure that you cover everything you want to ask. For amnesia, some basic questions to ask your doctor include:
What's the most likely cause of my symptoms?
Are there other possible causes for my symptoms?
What kinds of tests do I need? Do these tests require any special preparation?
Will my memory ever come back?
What treatments are available, and which do you recommend?
I have other health conditions. How can I best manage them together?
Do I need to restrict any activities?
Are there any brochures or other printed material that I can take home? What websites do you recommend?
In addition to the questions that you've prepared to ask your doctor, don't hesitate to ask questions during your appointment at any time that you don't understand something.
Your doctor is likely to ask you a number of questions, including:
When did you first notice your memory loss?
Did you experience any other symptoms at that time?
Were you involved in any trauma? For example, a car accident, violent collision in sports or an assault?
Did an illness or another event seem to trigger the memory loss?
Does anything help improve your memory?
What, if anything, appears to worsen your memory loss?
Are the memory problems intermittent or constant?
Has the memory loss stayed the same or is it getting worse?
Did the memory loss come on suddenly or gradually?
To diagnose amnesia, a doctor will do a comprehensive evaluation to rule out other possible causes of memory loss, such as Alzheimer's disease, other forms of dementia, depression or brain tumor.
The evaluation starts with a detailed medical history. Because the person with memory loss may not be able to provide thorough information, a family member, friend or another caregiver generally takes part in the interview as well.
The doctor will ask many questions to understand the memory loss. Issues that might be addressed include:
Type of memory loss — recent or long term
When the memory problems started and how they progressed
Triggering factors, such as head injury, stroke or surgery
Family history, especially of neurological disease
Drug and alcohol use
Other signs and symptoms, such as confusion, language problems, personality changes or impaired ability to care for self
History of seizures, headaches, depression or cancer
The physical examination may include a neurological exam to check reflexes, sensory function, balance, and other physiological aspects of the brain and nervous system.
The doctor will test the person's thinking, judgment, and recent and long-term memory. He or she will check the person's knowledge of general information — such as the name of the current president — as well as personal information and past events.
The memory evaluation can help determine the extent of memory loss and provide insights about what kind of help the person may need.
Imaging tests — including MRI and CT scan — may be ordered to look for damage or abnormalities in the brain. Blood tests can check for infection, nutritional deficiencies or other issues. An electroencephalogram may be ordered to look for the presence of seizure activity.
Treatment for amnesia focuses on techniques and strategies to help make up for the memory problem.
A person with amnesia may work with an occupational therapist to learn new information to replace what was lost, or to use intact memories as a basis for taking in new information.
Memory training may also include a variety of strategies for organizing information so that it's easier to remember and for improving understanding of extended conversation.
Many people with amnesia find it helpful to use smart technology, such as a smartphone or a hand-held tablet device. With some training and practice, even people with severe amnesia can use these electronic organizers to help with day-to-day tasks. For example, smartphones can be programmed to remind them about important events or to take medications.
Low-tech memory aids include notebooks, wall calendars, pill minders, and photographs of people and places.
No medications are currently available for treating most types of amnesia.
Amnesia caused by Wernicke-Korsakoff syndrome involves a lack of thiamin. Treatment includes replacing this vitamin and providing proper nutrition. Although treatment, which also needs to include alcohol abstinence, can help prevent further damage, most people won't recover all of their lost memory.
Researchers are investigating several neurotransmitters involved in memory formation, which may one day lead to new treatments for memory disorders. But the complexity of the brain processes involved makes it unlikely that a single medication will be able to resolve memory problems.
Living with amnesia can be frustrating for those with memory loss, and for their family and friends, too. People with more-severe forms of amnesia may require direct assistance from family, friends or professional caregivers.
It can be helpful to talk with others who understand what you're going through, and who may be able to provide advice or tips on living with amnesia. Ask your doctor if he or she knows of a support group in your area for people with amnesia and their loved ones.
If an underlying cause for the amnesia is identified, there are national organizations that can provide additional information or support for the individual and their families. Examples include:
The Alzheimer's Association (800-272-3900)
The Brain Injury Association of America (800-444-6443)
Because damage to the brain can be a root cause of amnesia, it's important to take steps to minimize your chance of a brain injury. For example:
Avoid excessive alcohol use.
Wear a helmet when bicycling and a seat belt when driving.
Treat any infection quickly so that it doesn't have a chance to spread to the brain.
Seek immediate medical treatment if you have any symptoms that suggest a stroke or brain aneurysm, such as a severe headache or one-sided numbness or paralysis.


 Вода позволяет организму быстрее избавляться от вредных веществ, а мышечным тканям организма работать с большей силой.
Вода позволяет организму быстрее избавляться от вредных веществ, а мышечным тканям организма работать с большей силой. Учитесь на протяжении всей своей жизни и ваш головной мозг будет вам благодарен!
Учитесь на протяжении всей своей жизни и ваш головной мозг будет вам благодарен! Планируете начать изучение иностранного языка?
Планируете начать изучение иностранного языка?